Chapter 546 Polycystic Ovary Syndrome and Hirsutism
Polycystic Ovary Syndrome
Etiology and Definition
Polycystic ovary syndrome (PCOS) is a common disorder of reproductive hormone dysfunction, often with associated metabolic abnormalities, that affects 5-8% of women of reproductive age. The disorder typically emerges in adolescence when a normal menstrual pattern is not established and there is clinical evidence of androgen excess. It is characterized by the triad of oligo-ovulation or anovulation, clinical or biochemical hyperandrogenism, and ovarian cysts (≥12 immature follicles) (the Rotterdam criteria). Various expert bodies prioritize these elements differently for establishing the diagnosis, and few require the presence of all 3. Hyperandrogenism with ovulatory dysfunction (with exclusion of other causes) is most often considered sufficient for diagnosis in the USA. Abnormalities commonly associated with PCOS include obesity, insulin resistance, and the metabolic syndrome, but the phenotype is variable (see  Table 546-1 on the Nelson Textbook of Pediatrics website at www.expertconsult.com).
Table 546-1 on the Nelson Textbook of Pediatrics website at www.expertconsult.com).

Pathology Pathogenesis and Genetics
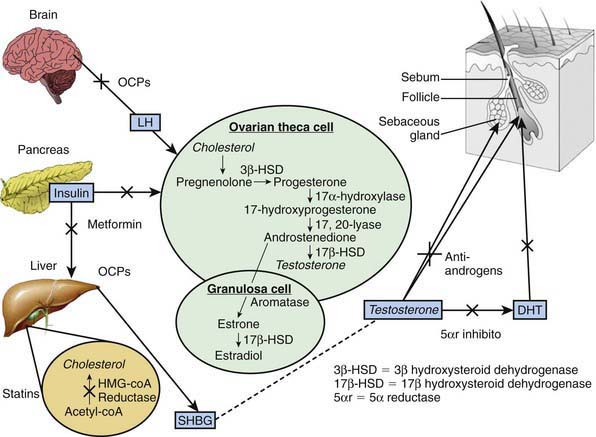
Gonadotropic dysregulation with increased luteinizing hormone (LH) pulsatility and abnormally high ratios of circulating LH to follicle-stimulating hormone (FSH) are found in many patients with PCOS. Increased ovarian production of androgen in response to LH and impaired folliculogenesis owing to lower FSH are attributed to this gonadotropic pattern. Abnormal regulation of gonadotropin-releasing hormone agonist (GnRH) and abnormal gonadotropin secretion more likely reflect the abnormal hormonal milieu of the syndrome than explain its origin (Fig. 546-1). An increased ratio of circulating levels of LH to FSH is not a diagnostic criterion for PCOS.
Clinical Manifestations
PCOS commonly becomes manifest as puberty progresses, but its onset can occur later during young adulthood. PCOS is a lifelong disorder (though with some evidence for amelioration with age or weight loss) (Table 546-2). Clinical hallmarks are menstrual abnormalities and manifestations of hyperandrogenism. Ovulation is typically irregular or absent, and menses are consequently irregular or absent. When they do occur, menses may be relatively normal in character as a consequence of a preceding ovulation. In many women, protracted periods of unopposed estrogen exposure without ovulation can terminate erratically in bleeding that is abnormally prolonged and/or heavy.
Table 546-2 LIFELONG HEALTH COMPLICATIONS
| PRENATAL OR CHILDHOOD | ADOLESCENCE, REPRODUCTIVE YEARS | POSTMENOPAUSAL |
|---|---|---|
| REPRODUCTIVE | ||
| Delayed menopause? | ||
| METABOLIC | ||
| Abnormal fetal growth | ||
| OTHER | ||
| Cardiovascular disease? | ||
From Norman RJ, Dewailly D, Legro RS, et al: Polycystic ovary syndrome, Lancet 370:685–696, 2007.
Laboratory Findings, Diagnosis, and Differential Diagnosis
The diagnosis of PCOS requires exclusion of disorders that would otherwise account for hyperandrogenism and anovulation. Serum 17-hydroxyprogesterone should be measured when there is clear androgen excess to screen for adult-onset 21-hydroxylase deficiency (Chapter 570
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


