Pneumothorax
Daniel J. Podberesky, MD
DIFFERENTIAL DIAGNOSIS
Common
Pulmonary Hypoplasia
Surfactant Deficiency Disease
Meconium Aspiration Syndrome
Pulmonary Interstitial Emphysema
Asthma
Cystic Fibrosis, Lung
Iatrogenic
Spontaneous
Trauma
Skin Fold (Mimic)
Less Common
Langerhans Cell Histiocytosis
Tuberous Sclerosis Complex
Ruptured Bulla/Blebs
Rare but Important
Metastatic Neoplasm
Infection
Marfan Syndrome
Ehlers-Danlos Syndrome
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
History is extremely helpful in determining possible source of pneumothorax
Is there history of trauma? asthma? recent instrumentation?
Appearance of pneumothorax depends on position of patient and amount of pleural gas
In supine patient, air collects anteromedially
Sharp, well-delineated cardiac and mediastinal borders
In upright patient, air collects laterally and apically
Radiolucent space lacking pulmonary vascular markings
White pleural line visible
Size of pneumothorax difficult to accurately estimate on chest x-ray
Signs of tension pneumothorax
Depressed/inverted hemidiaphragm
Contralateral shift of mediastinum
Expansion of spaces between ribs
Expiratory, decubitus, and cross-table lateral views may all aid in diagnosis in equivocal cases
Skin folds and pneumomediastinum can mimic pneumothorax
Helpful Clues for Common Diagnoses
Pulmonary Hypoplasia
Potter syndrome
Oligohydramnios related to fetal urinary system problems
Resultant pulmonary aplasia and typical abnormal facies
Pneumothorax may result from progressive air leaks &/or mechanical ventilation
Surfactant Deficiency Disease
Premature neonates
Reticulogranular opacities
Air leak from alveolar rupture can lead to pneumothorax
Meconium Aspiration Syndrome
History of meconium-stained amniotic fluid helpful
Coarse interstitial and patchy opacities
Hyperinflation
Pneumothorax may result from air-trapping and alveolar rupture
Pulmonary Interstitial Emphysema
Premature neonates
Barotrauma from mechanical ventilation
Reticular and cystic opacities
Alveolar rupture results in pneumothorax
Asthma
Airway narrowing and mucous plugging leads to air-trapping and alveolar rupture
History of asthma exacerbation helpful
Hyperinflated lungs
Cystic Fibrosis, Lung
Chronic lung disease can lead to airway obstruction and alveolar rupture
Superimposed infection increases pneumothorax risk
Pneumothorax indicates poor prognosis
Bronchiectasis, bronchial wall thickening, mucus plugging, hyperinflation, prominent hila
Iatrogenic
Mechanical ventilation
Instrumentation, such as central line placement or thoracentesis
Postoperative patients
History helpful
Spontaneous
Diagnosis of exclusion
No distinguishing radiologic features
Trauma
Pneumothorax may result from acute blunt or penetrating trauma
May also result from rupture of pneumatocele from old trauma
Motor vehicle crashes, falls, sports injuries
Other signs of trauma
Fractures
Pulmonary contusions
Mediastinal injuries
Pleural effusions
Skin Fold (Mimic)
Frequently seen in neonates in NICU
Can be difficult to differentiate from pneumothorax
Linear interface with Mach line
No white pleural line
Consider decubitus or cross-table lateral views in equivocal cases
Helpful Clues for Less Common Diagnoses
Langerhans Cell Histiocytosis
Small pulmonary nodules and parenchymal lung cysts
Apical reticulonodular pattern
Lung cysts may rupture and result in pneumothorax
Tuberous Sclerosis Complex
Lymphangioleiomyomatosis
Small parenchymal cysts
Chylous pleural effusion
Pneumothorax in ˜ 70%
Ruptured Bulla/Blebs
Small pleural blebs and parenchymal bulla may spontaneously rupture and lead to pneumothorax
CT can be very helpful in these cases
Helpful Clues for Rare Diagnoses
Metastatic Neoplasm
Pneumothorax may occur in presence of metastases, especially when present on pleural surface
Seen in children with osteosarcoma and Wilms tumor
Infection
Any infection that causes alveolar destruction can lead to pneumothorax
Particularly seen with tuberculosis and Pneumocystis infection
Marfan Syndrome
Autosomal dominant connective tissue disorder
At risk for spontaneous pneumothorax
Look for associated findings
Aortic aneurysms
Kyphoscoliosis
Arachnodactyly
Ehlers-Danlos Syndrome
Connective tissue disorder
At risk for spontaneous pneumothorax
Image Gallery
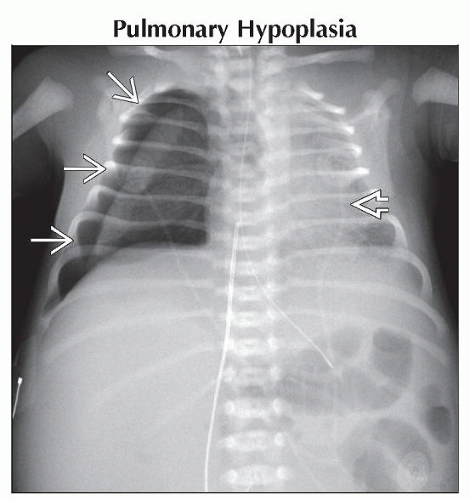 Frontal radiograph in this neonate with Potter syndrome shows a moderate right pneumothorax  . Note the shift of cardiomediastinal silhouette to the left . Note the shift of cardiomediastinal silhouette to the left  , evidence of a tension component. , evidence of a tension component. |
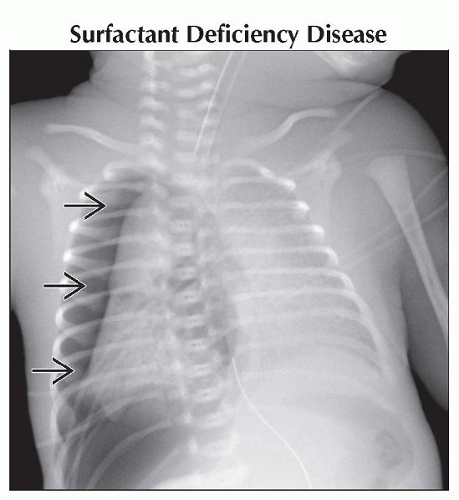 Frontal radiograph shows a large right-sided tension pneumothorax  in this premature neonate with surfactant deficient disease. Note the granular opacities throughout the lungs. in this premature neonate with surfactant deficient disease. Note the granular opacities throughout the lungs. |
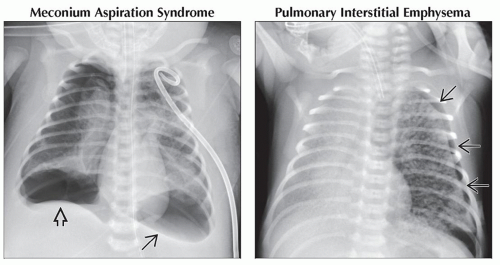 (Left) Frontal radiograph shows bilateral pneumothoraces in this neonate with meconium aspiration. Note the bilateral, coarse, interstitial lung opacities. The left pneumothorax is loculated
 & the right pneumothorax is under tension with depression of the diaphragm & the right pneumothorax is under tension with depression of the diaphragm  . (Right) Frontal radiograph shows a left pneumothorax . (Right) Frontal radiograph shows a left pneumothorax  in this premature neonate with pulmonary interstitial emphysema. Note diffuse, coarse, reticular opacities. in this premature neonate with pulmonary interstitial emphysema. Note diffuse, coarse, reticular opacities.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|