Pediatric Vascular Radiology
QUESTIONS
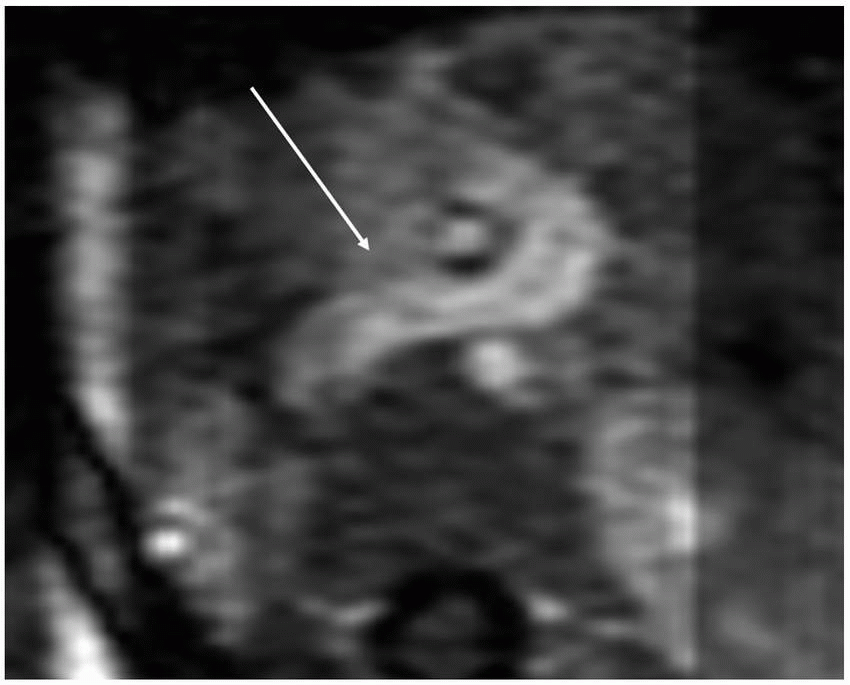
1 A 9-day-old presents with history of congenital stridor. An upper GI was performed (Fig. A). The most likely diagnosis is:
|

A. Pulmonary artery sling
B. Right arch with aberrant left subclavian
C. Tracheomalacia
D. Esophageal stenosis
View Answer
1 Answer A. A pulmonary artery sling causes an anterior impression on the esophagus (arrow) and a posterior impression on the trachea because of the left pulmonary artery passing between the trachea and esophagus (arrow in B). The left pulmonary artery arises from the posterior aspect of the right pulmonary artery. This condition occurs because of the obliteration of the primitive left sixth aortic arch.
A right arch with an aberrant left subclavian artery would produce a posterior impression on the esophagus, not an anterior impression.
Tracheomalacia is a condition where there is flaccidity of the airway wall and supporting cartilage. On imaging, there is collapse of the tracheal lumen most pronounced during expiration or coughing. This condition is associated with vascular rings such as pulmonary artery sling but is not demonstrated on this image.
Single-contrast barium upper gastrointestinal study demonstrates an anterior impression on the esophagus (arrow in A). There is no evidence of significant esophageal narrowing.
|

References: Lee EY, Dorkin H, Vargas SO. Congenital pulmonary malformations in pediatric patients: review and update on etiology, classification, and imaging findings. Radiol Clin N Am 2011;49(5):921-948.
Yedururi S, Guillerman P, Chung T, et al. Multimodality imaging of tracheobronchial disorders in children. Radiographics 2008;28(3):e29. doi:http://dx.doi.org/10.1148/rg.e29.
2 The following would reduce the dose to the child when performing the upper GI examination:
A. Use of an antiscatter grid
B. Reducing the magnification
C. Increasing the source to skin distance
D. Increasing the pulse rate
View Answer
2 Answer B. When the magnification increases, the field of view becomes smaller. Unfortunately, when the field of view becomes smaller and the magnification increases, the dose also increases. Reducing the magnification or enlarging the field of view will therefore decrease the radiation dose.
The antiscatter grid attenuates scattered radiation. Given that detection of this scattered radiation decreases image quality, it is often necessary to use the grid in larger patients. With removal of the scattered radiation, the primary dose of radiation must be increased to replace the scattered dose at the image receptor. In pediatric patients, the smaller body produces less scatter, and therefore, use of a grid only minimally improves image quality. Children under the age of 3 to 5 years generally can be imaged without the grid with similar image quality.
Decreasing the source to skin distance (SSD) will decrease the dose to the child. The inverse square law states that the intensity of radiation of the beam is inversely proportional to the square of the SSD. Because of this, decreasing the SSD will decrease the dose to the child, and increasing the SSD will increase the dose to the child.
The pulse rate is the number of fluoroscopic images the fluoroscopy machine creates per second. Increasing the pulse rate would increase the number of images per second and therefore increase the dose. Decreasing the pulse rate would decrease the number of images per second and decrease the dose.
Reference: Hernanz-Schulman M, Strauss K, Bercha IH. Fluoroscopy and radiation safety content for radiologists. http://www.imagegently.org/Portals/6/Radiologists/Background4radiologists.pdf
3 Concerning this diagnosis, a type II is classified as having the following characteristic:
A. Carina in a normal location at the level of T4 to T5
B. Low carina at the level of T6
C. High carina at the level of T3
D. Tracheal bronchus
View Answer
3 Answer B. A type II pulmonary artery sling is characterized by a low position of the carina at the level of T6. A type II pulmonary artery sling is associated with long-segment tracheal stenosis, a T-shaped carina, and a bridging bronchus.
Types of Pulmonary Artery Slings | ||||
|---|---|---|---|---|
|
Reference: Lee EY, Dorkin H, Vargas SO. Congenital pulmonary malformations in pediatric patients: review and update on etiology, classification, and imaging findings. Radiol Clin N Am 2011;49(5):921-948.
4 A right and left renal angiogram was performed on a 15-year-old female. What is the most likely diagnosis?
|

A. Autosomal dominant polycystic kidney disease
B. Atherosclerosis
C. Fibromuscular dysplasia
D. Segmental arterial mediolysis
View Answer
4 Answer C. Right and left renal angiograms demonstrate a normal right main renal artery but an early upper pole branch with irregular narrowing and a small aneurysm (arrow in A). The left main renal artery also has irregular stenosis and two small aneurysms (arrows in B). These findings are most compatible with fibromuscular dysplasia, particularly in this age group. Fibromuscular dysplasia is a nonatherosclerotic disease involving medium-sized vessels, most commonly the renal and extracranial carotid and vertebral arteries. Percutaneous transluminal renal angioplasty is the treatment of choice for renal fibromuscular dysplasis.
|

References: Meuse MA, Turba UC, Sabri SS, et al. Treatment of renal artery fibromuscular dysplasia. Tech Vasc Interv Radiol 2010;13:126-133.
O’Connor SC, Gornik HL. Recent developments in the understanding and management of fibromuscular dysplasia. J Am Heart Assoc 2014;3(6):e001259. doi:10.1161/JAHA.114.001259.
5 Of the following choices, what is the most common presenting sign of the disease in Question 4?
A. Chest pain
B. Headache
C. No presenting signs or symptoms
D. Hypertension
View Answer
5 Answer D. The most common presenting sign of fibromuscular dysplasia is hypertension followed by headache.
Most Common Presenting Signs and Symptoms of Fibromuscular Dysplasia | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Reference: O’Connor SC, Gornik HL. Recent developments in the understanding and management of fibromuscular dysplasia. J Am Heart Assoc 2014;3(6):e001259. doi:10.1161/JAHA.114.001259.
6 The most common subtype of this disease in Question 4 is the following:
A. Medial
B. Perimedial
C. Intimal
D. Serosal
View Answer
6 Answer A. The most common histopathologic subtypes of fibromuscular dysplasia are medial (70%), perimedial (15% to 25%), and intimal fibrodysplasia (1% to 2%). Both medial and perimedial fibrodysplasia tend to develop stenosis and aneurysms, whereas intimal fibrodysplasia develops smooth focal or tubular narrowing.
Reference: Meuse MA, Turba UC, Sabri SS, et al. Treatment of renal artery fibromuscular dysplasia. Tech Vasc Interv Radiol 2010;13:126-133.
7 The indications for percutaneous intervention in a patient with the disease in Question 4 include which of the following?
A. Resistant hypertension
B. Intolerance to hypertensive medications
C. Renal impairment
D. Noncompliance with hypertensive medications
E. A and C only
F. All of the above
View Answer
7 Answer F. Per the American College of Cardiology, the indications for percutaneous intervention in fibromuscular dysplasia include resistant hypertension, intolerance to antihypertensive medications, noncompliance with antihypertensive medications, and renal impairment. Other reasons for intervention are renal artery dissection and renal artery aneurysm.
References: Meuse MA, Turba UC, Sabri SS, et al. Treatment of renal artery fibromuscular dysplasia. Tech Vasc Interv Radiol 2010;13:126-133.
O’Connor SC, Gornik HL. Recent developments in the understanding and management of fibromuscular dysplasia. J Am Heart Assoc 2014;3(6):e001259. doi:10.1161/JAHA.114.001259.
8 A 2-day-old presents with history of a two-vessel cord and Williams syndrome. Which of the following are TRUE?
|

A. The infrarenal aorta is decreased in caliber.
B. The infrarenal aorta is enlarged in caliber.
C. The superior mesenteric artery is normal in caliber.
D. The superior mesenteric artery is decreased in caliber.
View Answer
8 Answer A. This patient has narrowing of the infrarenal aorta (arrows) consistent with middle aortic syndrome. The etiologies of this disorder include genetic causes such as Williams syndrome, Alagille syndrome, and neurofibromatosis. Additionally, vasculitis such as Takayasu arteritis and intrauterine infection such as rubella have been associated with this disorder.
|

References: Kim SM, Jung IM, Min SI, et al. Surgical treatment of middle aortic syndrome with takayasu arteritis or midaortic dysplastic syndrome. Eur J Endovasc Surg 2015;50:206-212.
Rumman RK, Nickel C, Matsuda-Abedini M, et al. Disease beyond the arch: a systemic review of middle aortic syndrome in childhood. Am J Hypertens 2015;28:833-846.
9 In the pediatric population, which is the first-line imaging modality to evaluate the disorder shown in Question 8?
A. Ultrasound with Doppler
B. Contrast-enhanced MRI
C. Contrast-enhanced CT
D. Subtraction angiography
View Answer
9 Answer A. Given the lack of ionizing radiation and the ability to perform without sedation, ultrasound with Doppler is the imaging modality of choice to initially evaluate a child with suspected middle aortic syndrome.
10 A commonly occurring collateral pathway to supply the lower extremities in the disorder shown in Question 8 is:
A. Intercostal arteries to inferior mesenteric artery to hemorrhoidal arteries to external iliac arteries
B. Intercostal arteries to inferior mesenteric artery to infrarenal abdominal aorta
C. Superior mesenteric artery to inferior mesenteric artery to hemorrhoidal arteries to external iliac arteries
D. Superior mesenteric artery to inferior mesenteric artery to infrarenal abdominal aorta
View Answer
10 Answer C. The most commonly occurring collateral pathways in abdominal aortoiliac stenosis are
1. Superior mesenteric artery to inferior mesenteric artery to hemorrhoidal arteries to external iliac arteries
2. Intercostal, subcostal, and lumbar arteries to superior gluteal and iliolumbar arteries to internal iliac arteries to external iliac arteries
3. Intercostal, subcostal, and lumbar arteries to circumflex arteries to external iliac arteries
Reference: Sebastia C, Quiroga S, Boye R, et al. Aortic stenosis: spectrum of diseases depicted at multisection CT. Radiographics 2003;23:S79-S91.
11 An 18-month-old with elevated liver function tests presents for MRI following abnormality noted on recent abdominal sonogram. The following axial and volumerendered images were obtained.
|

The most likely explanation for the prominent vessel extending below the SMA axis is:
A. Arteriovenous fistula
B. Aneurysmal dilatation of the left renal vein
C. Congenital portosystemic shunt
D. Interrupted IVC
View Answer
11 Answer C. There is connection of the splenic and superior mesenteric vein (arrow) to the inferior vena cava consistent with a congenital extrahepatic portosystemic shunt. This is a condition in which the portomesenteric blood drains into a systemic vein therefore bypassing the liver.
|
References: Alonso-Gamarra E, Parrion M, Perez A, et al. Clinical and radiologic manifestations of congenital extrahepatic portosystemic shunts: a comprehensive review. Radiographics 2011;32:707-722.
Kobayashi N, Niwa T, Kirikoshi H, et al. Clinical classification of congenital extrahepatic portosystemic shunts. Hepatol Res 2010;40:585-593.
12 What is the most likely classification of the abnormality shown in Question 11?
A. Type 1
B. Type 2
C. Type 3
D. Type 4
View Answer




12 Answer B. Congenital portosystemic shunts are initially classified as intrahepatic or extrahepatic. In this case, the abnormal connection is extrahepatic. Extrahepatic shunts are classified into type 1 where there is absence of the intrahepatic portal venous supply or type 2 in which the intrahepatic portal venous supply is present. In this case, no portal vein is present, so it is a type 2 extrahepatic portosystemic shunt.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
