endometriotic implants just as endogenous endometrial cells may. Further evidence demonstrates that endometriotic implants are populated by bone marrow-derived stem cells. This stem cell theory would also explain cases of endometriosis at sites outside the peritoneal cavity; endometriosis at distant sites may arise from stem cells.
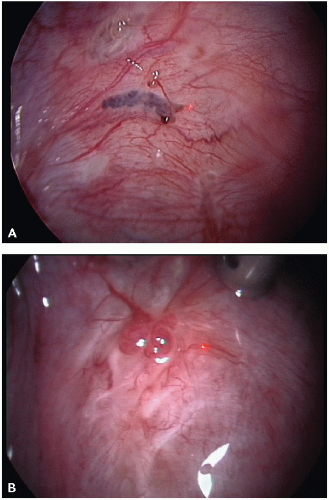 FIGURE 10.1 Typical and subtle endometriotic lesions on peritoneum. A: Typical black-puckered lesions with hypervascularization and orange polypoid vesicles. B: Red polypoid lesions with hypervascularization. (Photographs kindly donated by Dr. Christel Meuleman, Leuven University Fertility Center, Leuven University Hospitals, Leuven, Belgium. From Berek JS, ed. Berek & Novak’s Gynecology. 14th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
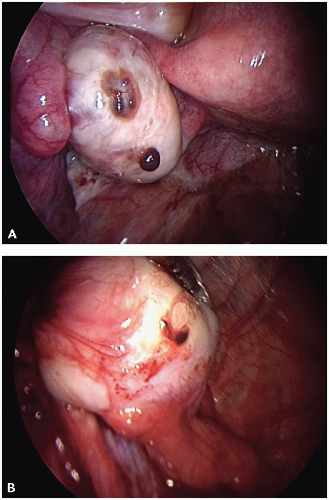 FIGURE 10.2 Ovarian endometriosis. A: Superficial ovarian endometriosis. B: Superficial ovarian endometriosis and endometrioma laparoscopic image prior to adhesiolysis. (Photographs kindly donated by Dr. Christel Meuleman, Leuven University Fertility Center, Leuven University Hospitals, Leuven, Belgium. From Berek JS, ed. Berek & Novak’s Gynecology. 14th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
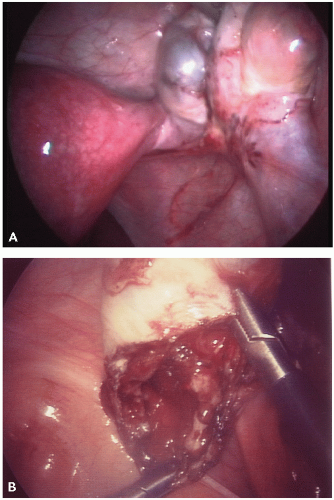 FIGURE 10.3 A: Laparoscopic image of uterus and right ovary with dark endometrioma. B: Ovarian endometriotic cystectomy. (From Berek JS. Berek & Novak’s Gynecology. 14th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
have laparoscopy are found to have endometriosis, and among adolescents with chronic pelvic pain that do not respond to oral contraceptives or NSAIDs who undergo laparoscopy, endometriosis is found in 50 to 70% of cases. Adolescents with endometriosis often have both acyclic and cyclic pain. The least common pain presentation among adolescents is isolated cyclic pain, which is in contrast to adults with endometriosis who commonly have cyclical pain.
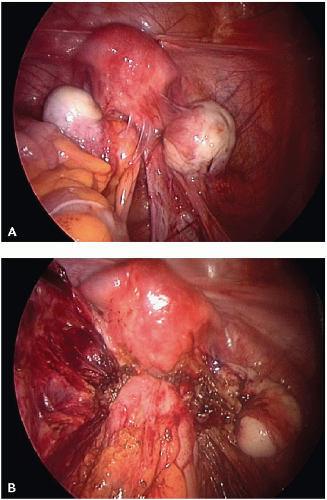 FIGURE 10.4 Laparoscopic excision of deep endometriosis from the cul de sac. A: Extensive endometriosis with deep nodule at the right uterosacral ligament masked by adhesions. B: Deep nodule is still present in dense adhesion between rectum and uterosacral ligaments. (Photographs kindly donated by Dr. Christel Meuleman, Leuven University Fertility Center, Leuven University Hospitals, Leuven, Belgium. From Berek JS. Berek & Novak’s Gynecology. 14th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
TABLE 10.1 Symptoms of Endometriosis | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
cancer, is elevated in endometriosis and has been found to have a diagnostic specificity greater than 90% and sensitivity of 50%.29 In one series of 685 women undergoing surgery for endometriosis, the mean serum CA-125 levels in stage I, II, III, and IV disease were 19, 40, 77, and 182 IU/mL, respectively.30 Levels greater than 100 IU/mL were usually associated with extensive adhesions or a ruptured endometrioma. Other conditions that increase CA-125 levels are pelvic inflammatory disease, leiomyomas, pregnancy, cirrhosis, and appendicitis (see Table 10.2 for a listing of conditions associated with elevated levels of CA-125).
TABLE 10.2 Conditions Associated With Elevated Serum CA-125 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
of endometriosis. Additional surgery may be indicated in women with known severe disease who desire fertility, and assisted reproductive techniques may follow surgery. No studies have directly compared surgical versus medical treatment for endometriosis (see Table 10.3 for a list of treatment options for endometriosis).
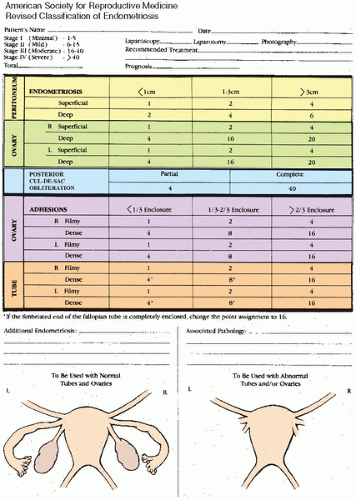 FIGURE 10.5 Revised American Society for Reproductive Medicine classification. (From Schenken R, Guzick D. Revised endometriosis classification: 1996. Fertil Steril. 1997;67:815-816.) |
in pregnancy, starting a combination oral contraceptive may be beneficial regardless of symptoms to prevent further progression of disease.
TABLE 10.3 Treatment Options for Endometriosis-Associated Pain | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 10.4 Medical Therapy Options and Dosages for Dysmenorrhea | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
controlled trials on OCPs for endometriosis. All, including the Cochrane Review, have found OCPs to be more effective than placebo and as effective as GnRH analogues and danazol.42, 43, 44 Low-dose OCPs have also been shown to decrease endometriosis pain symptoms.43 Side effects from OCPs include nausea, breast tenderness, and irregular vaginal bleeding. Contraindications should be reviewed prior to prescribing especially any history of thromboembolic events. There is no conclusive evidence that one OCP formulation is better than another.
TABLE 10.5 Drugs Used for the Treatment of Endometriosis | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


