likely to have publicly funded health care coverage but are at high risk of being underinsured.9 Women with disabilities are less likely to be married and are at higher risk for social isolation. Trouble accessing transportation is a major problem for many people with disabilities and can lead to geographic isolation. Many women with disabilities are unable to drive or cannot afford an accessible vehicle for personal use. Public transportation may be unavailable or difficult to access. Paratransit services, when available, are frequently unreliable.10
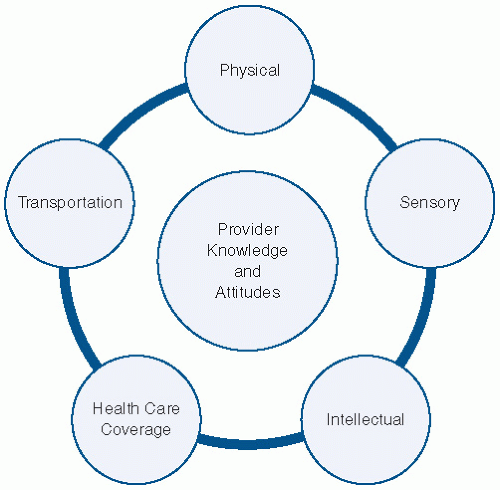 FIGURE 26.1 Barriers to care. (Adapted from American College of Obstetricians and Gynecologists. Reproductive health care for women with disabilities. Interactive site for clinicians serving women with disabilities. http://www.acog.org/departments/dept_notice.cfm?recno=38&bulletin=4526. Accessed December 5, 2013.) |
TABLE 26.1 Selected Disability Measures, Noninstitutionalized Females Ages 5 Years and Older, United States, 2006 | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
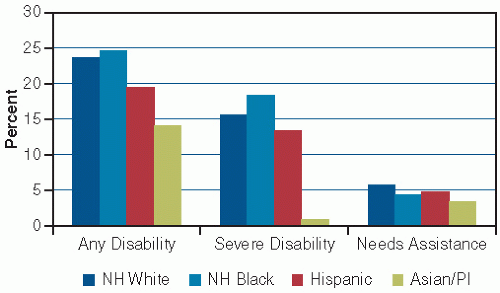 FIGURE 26.2 Disability prevalence among women age 15 years and older, by severity and race/ethnicity, 2002. Disability was defined as difficulty performing functional activities (e.g., seeing, walking), difficulty with activities of daily living (e.g., bathing, eating), difficulty with instrumental activities of daily living (e.g., managing money and bills, going outside the home), or presence of a learning disability or other mental or emotional condition. Severe disability was defined as use of a mobility aid; inability or need for assistance to perform one or more functional activities, activities of daily living, or instrumental activities of daily living; mental retardation, another developmental disability, or Alzheimer disease; a mental or emotional condition that seriously interfered with everyday activities; or limitation in the ability to work around the house or remain employed. (Data from U.S. Census Bureau. Survey of Income and Program Participation. Washington, DC: U.S. Census Bureau; 2002.2) |
regulations. Owners of buildings in which offices are leased may be responsible for access improvements under the law in some cases. Whether removal of a physical barrier is readily achievable or not is judged on a case-by-case basis, taking into account the cost of the modification and the financial resources of the covered entity, among other things. Tax credits and incentives are available for businesses that incur expenses for removal of barriers or improving access to persons with disabilities (see http://www.ada.gov/archive/taxpack.htm for details).
Ensuring that there is at least one reserved accessible parking space and that there is a safe and barrier-free (i.e., no curbs or steps) path between the parking space and entrance.
Installing ramps to overcome architectural barriers. Ramps may be purchased or built and must include 12 inches of length for every 1-inches increase in elevation.
Enlarging door widths to at least 30 inches; 32- to 36-inches doorways are ideal.
Removing or adapting doorway thresholds that are not flush with the floor.
Ensuring that trash cans, plants, or other items do not block elevator call buttons.
Locating a building directory so it is visible from wheelchair height; using a font large enough to be read by people with vision impairment.
Installing a power door opener or a doorbell for use by people who cannot open a door independently.
Exchanging round doorknobs with “lever” door handles.
Having at least a portion of the reception desk lowered to wheelchair height.
Mailing long medical history and other intake forms to patients in advance.
Training reception staff to come around the desk to assist patients with check in, especially if the reception desk is not lowered. Offering assistance with completing forms in a private location.
Preserving a space for a wheelchair in the waiting area.
Clearing boxes, equipment, or other items from office hallways.
Allowing flexibility in scheduling to accommodate late arrivals related to transportation difficulties. Scheduling longer appointments to accommodate patients’ additional needs (e.g., assistance with forms,
undressing or transfer assistance, communication through an interpreter).
Inviting women with disabilities to assess office layout and practices and make suggestions for improvement.
methods of contraception difficult to use.9 In women with disabilities, symptoms of STIs may be unperceived or may be ascribed to a urinary tract infection without investigation, thus diagnosis is often delayed.17
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


