TABLE 22.1 Examples of Human Evidence That Documents Key Principles in Reproductive Environmental Health | ||||
|---|---|---|---|---|
|
immune system and blood-brain barrier.30 Reducing or eliminating exposure to environmental contaminants prior to conception is the most effective strategy for preventing adverse health consequences. Clinicians do not need to become experts in environmental and occupational health in order to fulfill this crucial role.
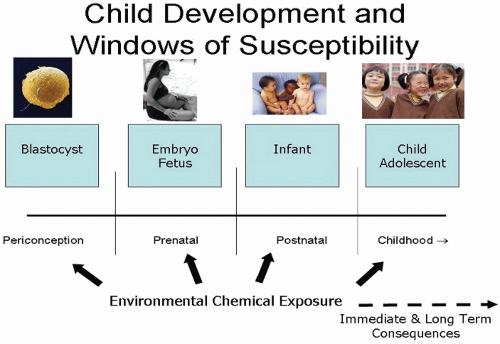 FIGURE 22.1 Windows of susceptibility. (Modified from Buck Louis GM, Gray LE Jr, Marcus M, et al. Environmental factors and puberty timing: expert panel research needs. Pediatrics. 2008;121[suppl 3]:S192-S207.) |
Animal studies clearly show that the in utero and neonatal developmental periods represent “critical windows” for nutrition and environmental exposures to impact later development.40 Other important features about the developmental origins of disease and dysfunction paradigm are:
The initiating in utero environmental insult can act alone or in concert with other environmental stressors;
There is a range of potential effects and latencies (including the potential to affect future generations);
Aberrant developmental programming can permanently alter gland, organ, or system potential;
TABLE 22.2 Selected Examples of Contaminants Linked to Reproductive, Fertility, or Developmental Problems | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
due to ethical considerations. Therefore, when making decisions about patient exposure to environmental and occupational exposure to chemicals, clinicians must rely on in vitro and in vivo studies for early warnings of adverse effects and human observational studies to assess the nature and extent of the damage.
TABLE 22.3 Percentage of U.S. Pregnant Women With Metals and Synthetic Chemicals Measured in Their Body* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
to daughter cells.63 Environmental modifications of gene expression can affect embryonic imprinting, cellular differentiation, and phenotypic expression.64 The most common epigenomic alterations are methylation of the DNA at cytosine with subsequent gene silencing or modification of the DNA histone support, which affects chromatin folding and attachment. Tight folding inhibits gene expression and lithe folding allows gene manifestation.64
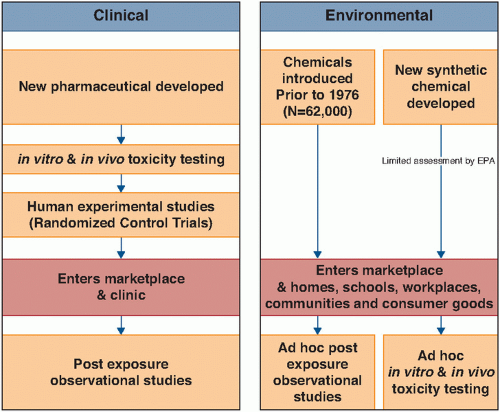 FIGURE 22.2 Comparison of streams of evidence in clinical and environmental health sciences. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


