Chapter 24 Obstetric operations
INDUCTION OF LABOUR
Induction of labour may be required to ‘rescue’ the fetus from a potentially hazardous intra-uterine environment in late pregnancy for a variety of reasons, or because continuation of the pregnancy is dangerous to the expectant mother. Indications for induction of labour are listed in Table 24.1.
Table 24.1 Indications for induction of labour: Australia
| Indication | Proportion of Inductions |
|---|---|
| Prolonged pregnancy (41 or more weeks) | 26% |
| Hypertensive disorders | 12% |
| Prelabour/prolonged rupture of membranes | 10% |
| Diabetes – pregestational and gestational | 7% |
| Intra-uterine growth restriction | 5% |
| Non-reassuring fetal status | 2% |
| Fetal death in utero (FDIU) | 1% |
| Blood group isoimmunization | 0.2% |
| Chorioamnionitis | 0.1% |
| Social induction | 16% |
| Others | 21% |
The method adopted depends on:
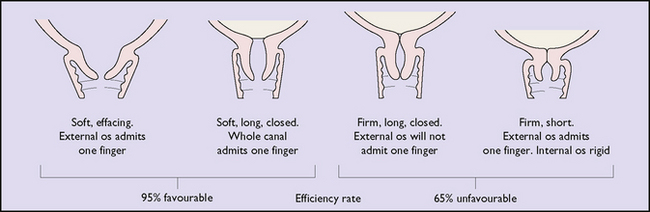
Fig. 24.1 The relationship between the condition of the cervix and success rate of surgical induction.
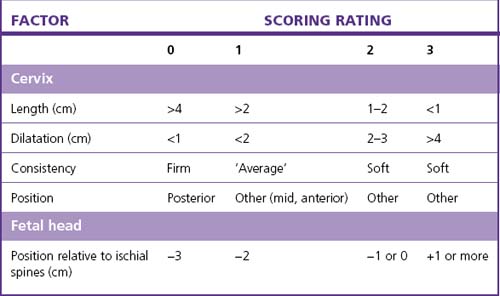
The highest rate of success, (i.e. that the induction is followed by a vaginal birth within 24 hours) occurs in a woman whose cervix is favourable and whose Bishop score is 5 or more (Table 24.2).
If the chances of success are evaluated as low, the doctor may recommend caesarean section.
Techniques of inducing labour
Induction of labour using drugs
Two agents are available: prostaglandins and oxytocin.
Prostaglandins
Three prostaglandins with different properties are used.
Surgical induction of labour (amniotomy)
The problems following amniotomy are:
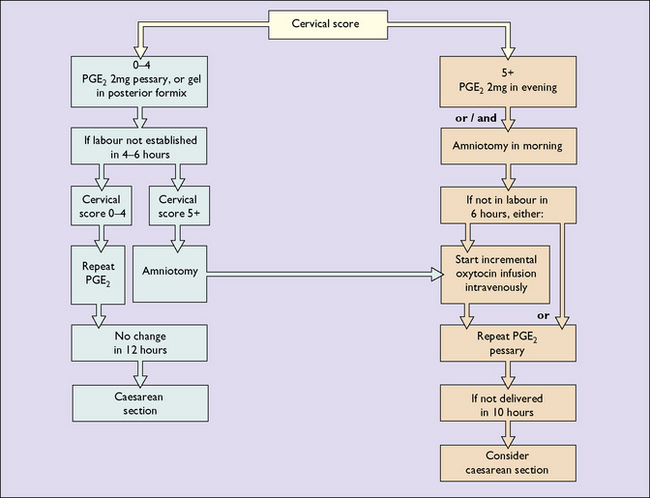
A suggested schema (flow chart) for the induction of labour is shown in Figure 24.2.
AUGMENTATION OF LABOUR
In cases where the quality of the uterine contractions is poor (see p. 174), their strength may be augmented by performing ARM and, if necessary, by setting up an incremental oxytocic infusion, or both.
INSTRUMENTAL DELIVERY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


