Chapter 41 Nutritional Requirements
Dietary Reference Intakes
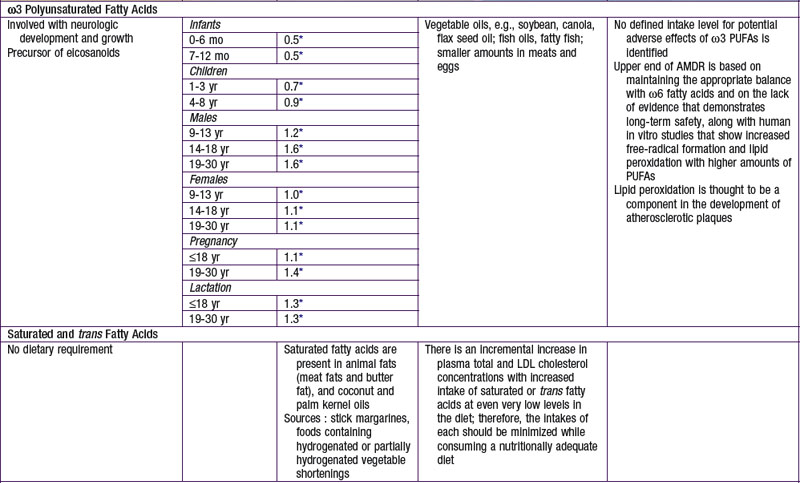
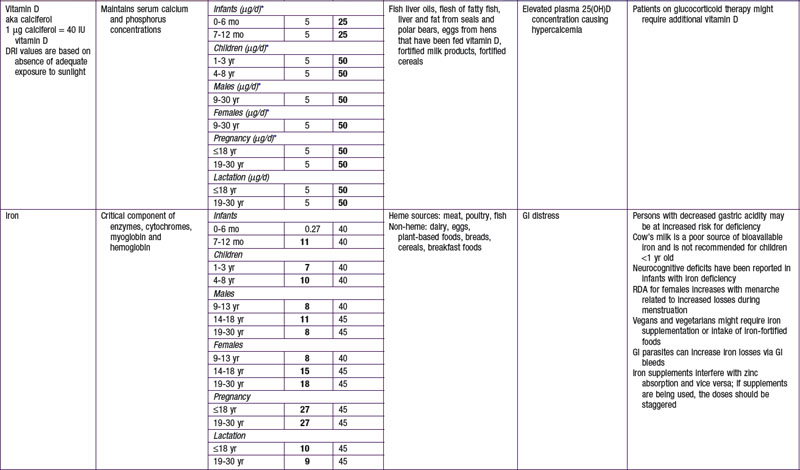
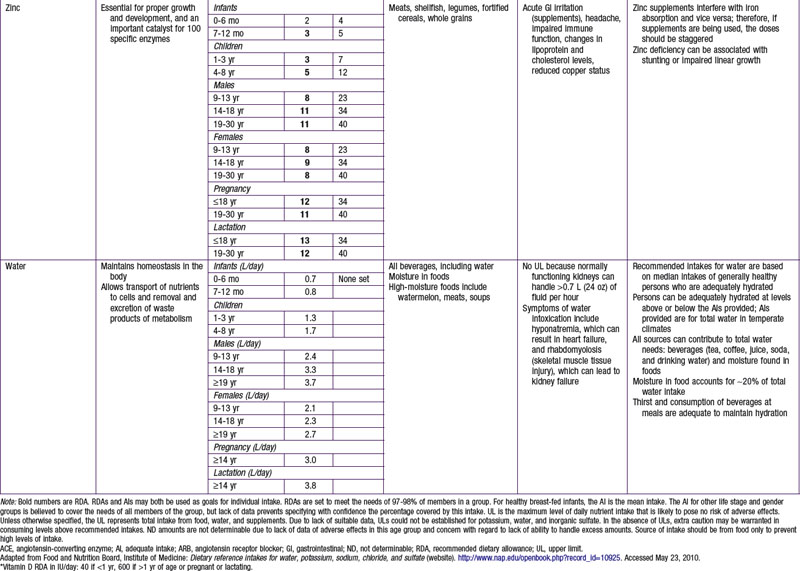
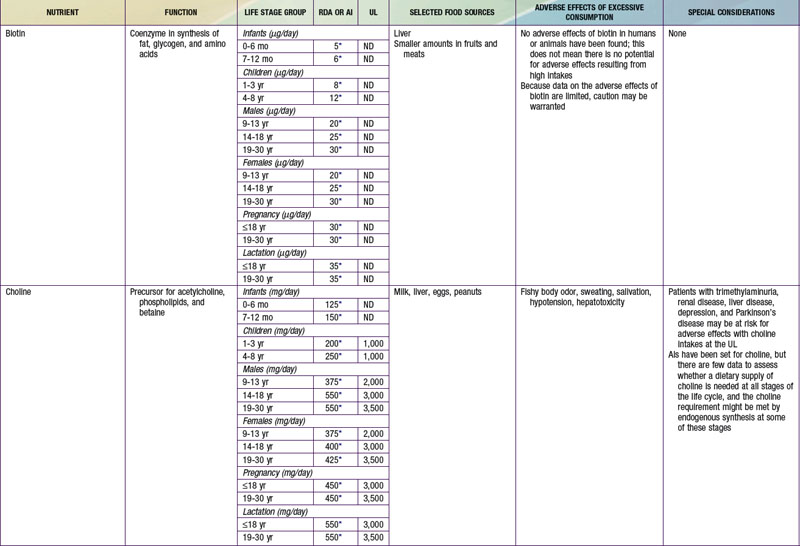
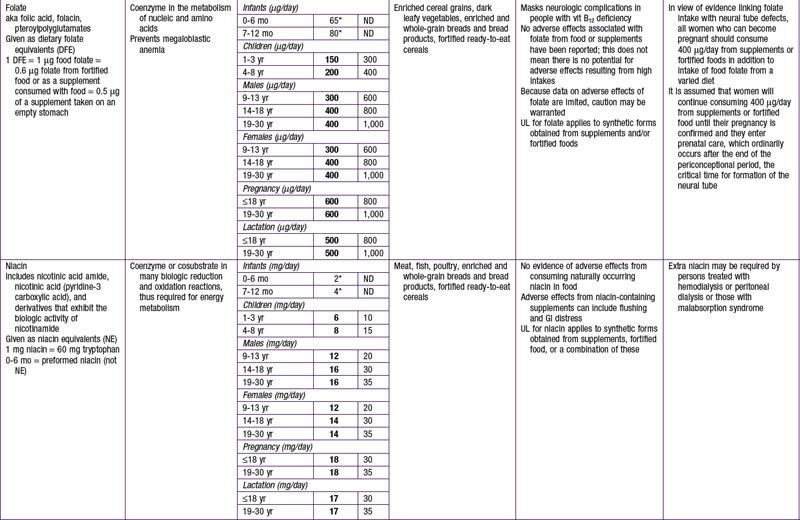
The dietary reference intake (DRI) has been established for most nutrients by the Food and Nutrition Board of the Institute of Medicine using a rigorous process of scientific evidence evaluation (Tables 41-1 to 41-8). The DRI provides guidance as to nutrient needs for individuals and groups across different life stages and by sex. The DRI replaces the former recommended dietary allowances (RDA).
Table 41-1 DEFINING THE DIETARY REFERENCE INTAKES
Table 41-2 EQUATIONS TO ESTIMATE ENERGY REQUIREMENT
| INFANTS AND YOUNG CHILDREN: EER (kcal/day) = TEE + ED | |
| 0-3 mo | EER = (89 × weight [kg] − 100) + 175 |
| 4-6 mo | EER = (89 × weight [kg] − 100) + 56 |
| 7-12 ms | EER = (89 × weight [kg] − 100) + 22 |
| 13-35 mo | EER = (89 × weight [kg] − 100) + 20 |
| CHILDREN AND ADOLESCENTS 3-18 yr: EER (kcal/day) = TEE + ED | |
| Boys | |
| 3-8 yr | EER = 88.5 − (61.9 × age [yr] + PA × [(26.7 × weight [kg] + (903 × height [m])] +20 |
| 9-18 yr | EER = 88.5 − (61.9 × age [yr] + PA × [(26.7 × weight [kg] + (903 × height [m])] +25 |
| Girls | |
| 3-8 yr | EER = 135.3 − (30.8 × age [yr] + PA [(10 × weight [kg] + (934 × height [m])] + 20 |
| 9-18 yr | EER = 135.3 − (30.8 × age [yr] + PA [(10 × weight [kg] + (934 × height [m])] + 25 |
ED, energy deposition; EER, estimated energy requirement; PA, physical activity quotient; TEE, total energy expenditure.
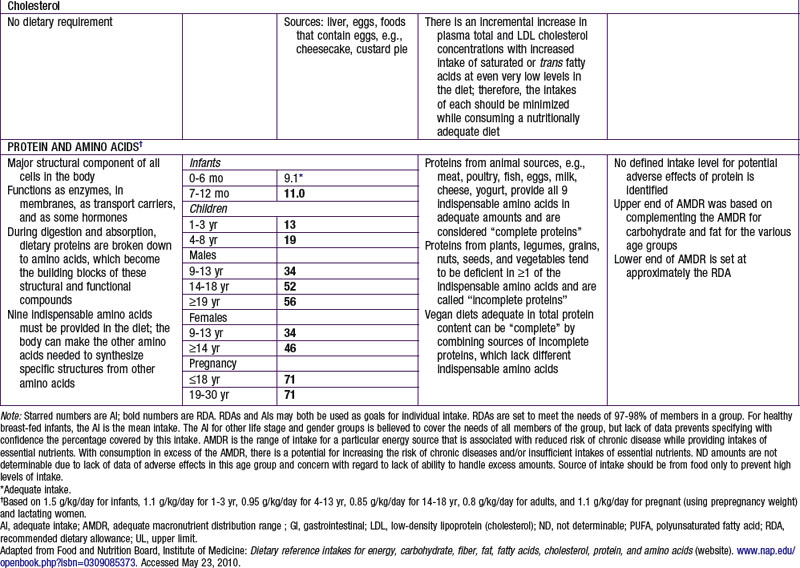
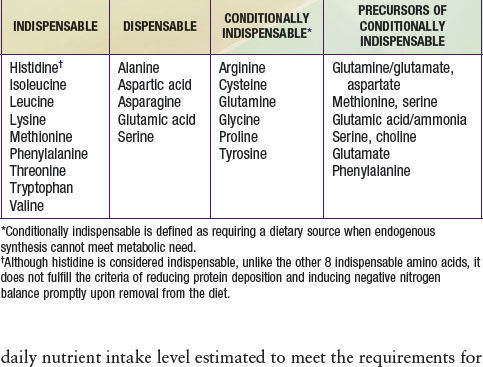
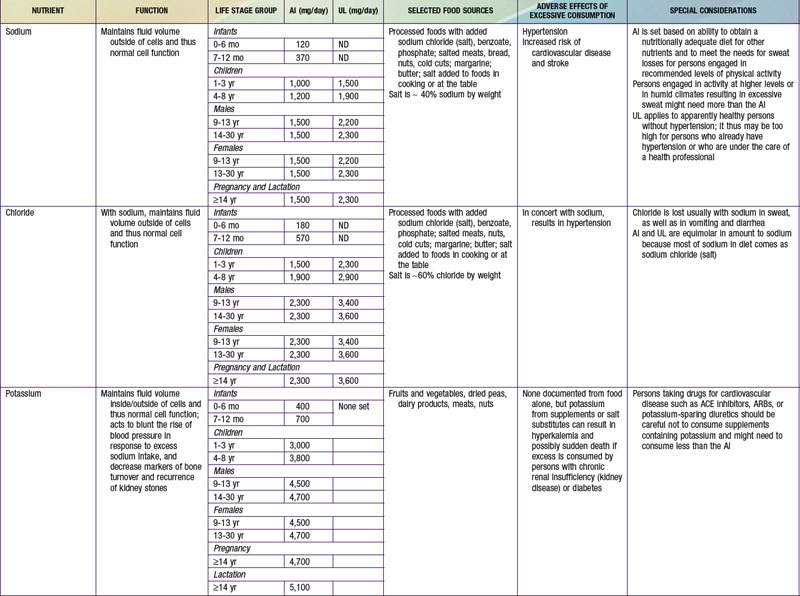
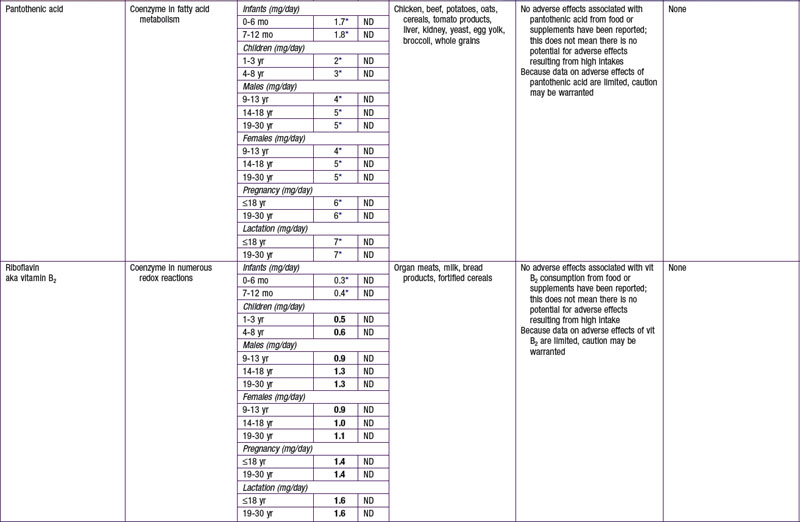
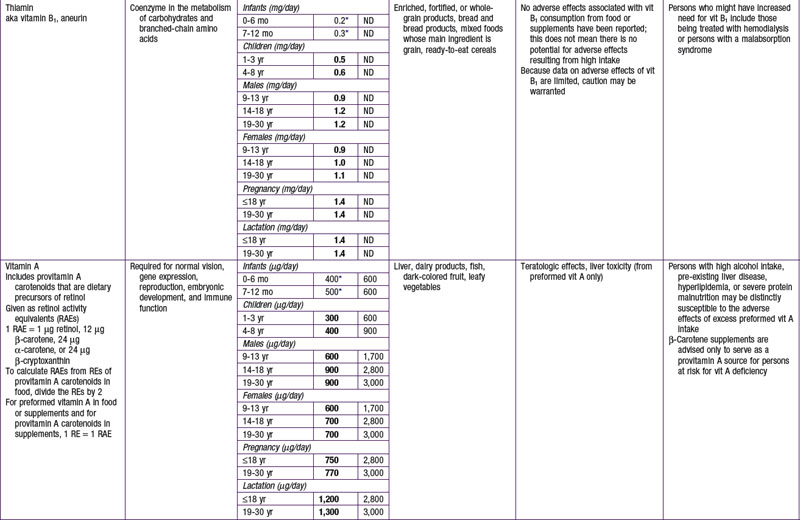
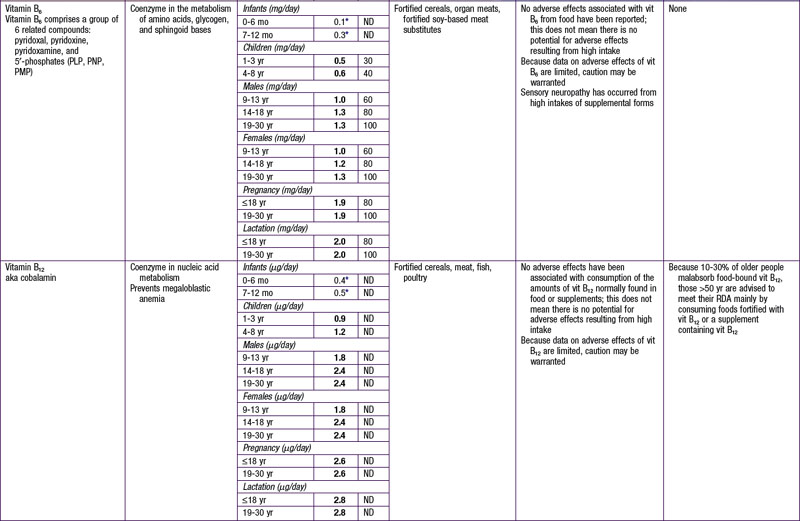
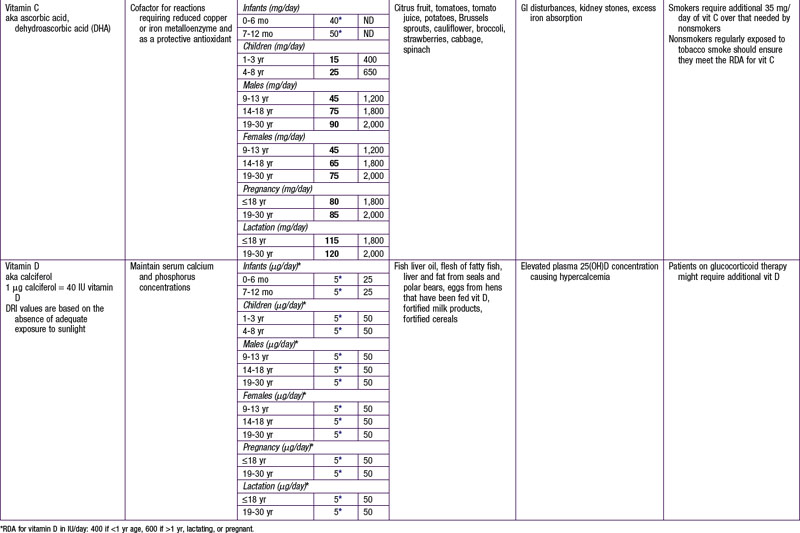

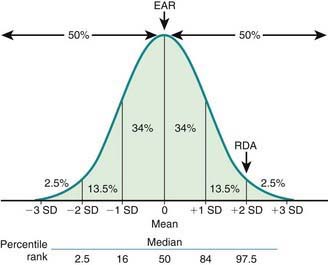
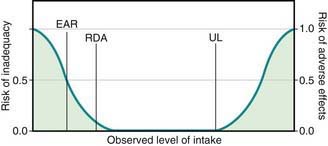
Key DRI concepts include the estimated average requirement (EAR), the recommended dietary allowance (RDA), and the tolerable upper limit of intake (UL) (Fig. 41-1). The EAR is the average daily nutrient intake level estimated to meet the requirements for 50% of the population, assuming normal distribution; the RDA is an estimate of the daily average nutrient intake to meet the nutritional needs of >97% of the individuals in a population, and it can be used as a guideline for individuals to avoid deficiency in the population. When an EAR cannot be derived, an RDA cannot be calculated; therefore, an adequate intake (AI) is developed as a guideline for individuals based on the best available data and scientific consensus. The UL denotes the highest average daily intake at which no adverse health effects are associated for almost all individuals in a particular group. The relationships among EAR, RDA, and UL are characterized in Figure 41-2.
Energy
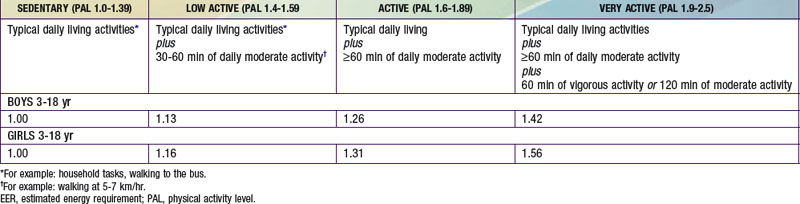
The estimated energy requirement (EER) is the average dietary energy intake predicted to maintain energy balance in a healthy individual of a defined group. The EER accounts for age, gender, weight, stature, and physical activity level (PAL) (see Tables 41-2 and 41-3). The Dietary Guidelines for Americans and the DRI recommend 60 min of moderately intense daily activity for children >2 yr of age to maintain a healthy weight and to prevent or delay progression of chronic noncommunicable diseases such as obesity and cardiovascular disease. The EER was determined based on empirical research in healthy persons at different physical activity levels, including levels different from the recommended levels. They do not necessarily apply to children with acute or chronic diseases. EER is estimated by equations that account for total energy expenditure as well as energy deposition for healthy growth. Note that the EER for infants, relative to body weight, are approximately twice those for adults, due to the increased metabolic rate and requirements for weight maintenance and tissue accretion affecting growth.
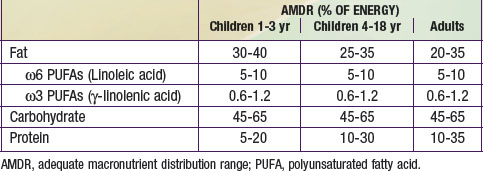
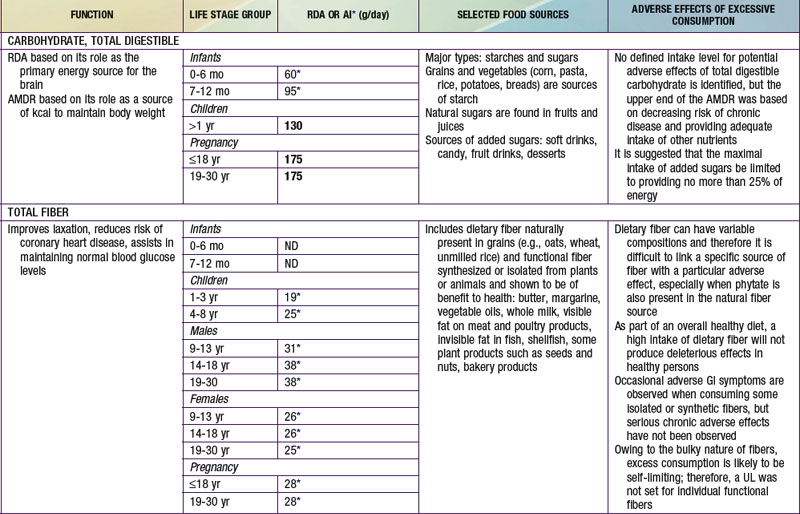
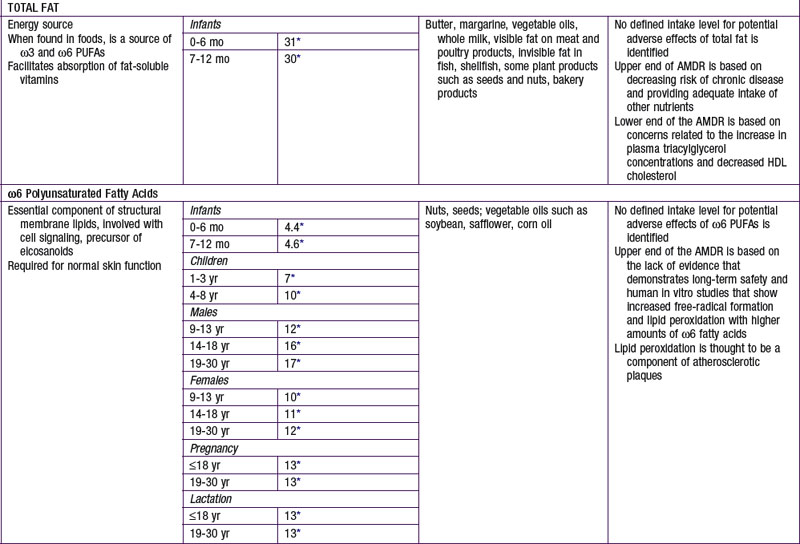
The nutrients that provide energy intake in the child’s diet are fats (∼ 9 kcal/g), carbohydrates (∼ 4 kcal/g), and proteins (∼ 4 kcal/g). They are referred to as macronutrients. Alcohol intake can also contribute to energy intake (∼ 7 kcal/g). The EER does not specify the relative energy contributions of carbohydrates, fats, or proteins. Once the minimal intakes of each of the respective macronutrients are attained to meet physiologic requirements and to achieve adequacy (sufficient protein intake to meet specific amino acid requirements), the remainder of the intake is used to meet energy requirements with some degrees of freedom and interchangeability among fats, carbohydrates, and proteins. This forms the basis for the acceptable macronutrient distribution ranges (AMDR) (see Table 41-4), expressed as a function of total energy intake. In the following sections, each macronutrient is reviewed.



