Chapter 536 Neuropathic Bladder
Neuropathic bladder dysfunction in children usually is congenital, generally resulting from neural tube defects or other spinal abnormalities. Acquired diseases and traumatic lesions of the spinal cord are less common. Central nervous system tumors, sacrococcygeal teratoma, spinal abnormalities associated with imperforate anus (Chapter 336), and spinal cord trauma also can result in abnormal innervation of the bladder and/or sphincter.
Neural Tube Defects
Neural tube defects, resulting from failure of the neural tube to close spontaneously between the 3rd and 4th wk in utero, result in abnormalities of the vertebral column that affect spinal cord function, including myelomeningocele and meningocele (Chapter 585). A few medical centers in the USA have been performing antenatal myelomeningocele closure, but follow-up studies of the urinary tract have not shown a definite improvement in lower urinary tract function.
Clinical Manifestations and Diagnosis
The most important urologic consequences of neuropathic bladder dysfunction associated with neural tube defects are urinary incontinence (Chapter 537), urinary tract infections (UTIs; Chapter 532), and hydronephrosis from vesicoureteral reflux or detrusor-sphincter dyssynergia. Pyelonephritis (Chapter 532) and renal functional deterioration (see Chapter 529) are common causes of premature death of affected patients.
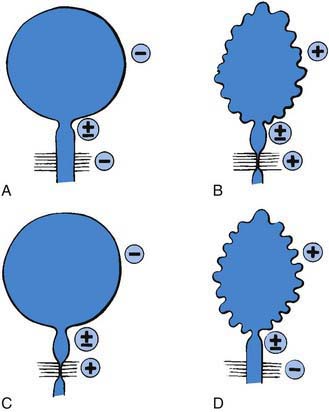
In the neonate, renal ultrasonography, assessment of postvoid residual urine volumes, and a voiding cystourethrogram are performed after closure of the myelomeningocele. About 10-15% of patients have hydronephrosis, and renal malformations are common; 25% have vesicoureteral reflux. A urodynamic study also should be performed. This study involves filling the bladder with saline, measuring the bladder volume and pressure, and assessing sphincter tone. During bladder filling, the bladder might show uninhibited (premature) contractions at low volumes, normal bladder volume with contraction at an appropriate volume, or atonia (lack of bladder contraction). Bladder compliance or elasticity also may be reduced. The sphincter can show normal tone with relaxation during bladder contraction, reduced or absent tone, or normal or increased tone that increases during bladder contraction (termed detrusor-sphincter dyssynergia) (Fig. 536-1).
Renal Damage
Renal damage usually results from failure of the sphincter to relax during a spontaneous bladder contraction. This dyssynergia results in functional obstruction of the bladder outlet, leading to high intravesical pressure, bladder muscle hypertrophy and trabeculation, and transmission of the high pressure into the upper urinary tracts, causing hydronephrosis (Fig. 536-2). Vesicoureteral reflux and UTI compound the problem. Treatment includes reduction of bladder pressure with anticholinergic drugs (oxybutynin, 0.2 mg/kg/24 hr in 2 or 3 divided doses) and clean intermittent catheterization every 3-4 hr. If there is vesicoureteral reflux or UTI, antimicrobial prophylaxis also is prescribed.




