Chapter 592 Neurodegenerative Disorders of Childhood
Neurodegenerative disorders of childhood encompass a large, heterogeneous group of diseases that result from specific genetic and biochemical defects, chronic viral infections, and varied unknown causes. Children with suspected neurodegenerative disorders were once subjected to brain and rectal (neural) biopsies, but with modern neuroimaging techniques and specific biochemical and molecular diagnostic tests, these invasive procedures are rarely necessary. The most important component of the diagnostic investigation continues to be a thorough history and physical examination. The hallmark of a neurodegenerative disease is regression and progressive deterioration of neurologic function with loss of speech, vision, hearing, or locomotion, often associated with seizures, feeding difficulties, and impairment of intellect. The age of onset, rate of progression, and principal neurologic findings determine whether the disease affects primarily the white or the gray matter. Upper motor neuron signs and progressive spasticity are the hallmarks of white matter disorders; convulsions, intellectual, and visual impairment that occur early in the disease course are the hallmarks of grey matter disorders. A precise history confirms regression of developmental milestones, and the neurologic examination localizes the process within the nervous system. Although the outcome of a neurodegenerative condition is usually fatal and available therapies are often limited in effect, it is important to make the correct diagnosis so that genetic counseling may be offered and prevention strategies can be implemented. Bone marrow transplantation and other novel therapies may prevent the progression of disease in certain presymptomatic individuals. For all conditions in which the specific enzyme defect is known, prevention by prenatal diagnosis (chorionic villus sampling or amniocentesis) is possible. Carrier detection is also often possible by enzyme assay. Table 592-1 summarizes selected inherited neurodegenerative and metabolic disorders by their age of onset.
Table 592-1 NEUROMETABOLIC CONDITIONS ASSOCIATED WITH DEVELOPMENTAL REGRESSION
| AGE AT ONSET (yr) | CONDITIONS | COMMENTS |
|---|---|---|
| <2, with hepatomegaly | Fructose intolerance | Vomiting, hypoglycemia, poor feeding, failure to thrive (when given fructose) |
| Galactosemia | Lethargy, hypotonia, icterus, cataract, hypoglycemia (when given lactose) | |
| Glycogenosis (glycogen storage disease) types I-IV | Hypoglycemia, cardiomegaly (type II) | |
| Mucopolysaccharidosis types I and II | Coarse facies, stiff joints | |
| Niemann-Pick disease, infantile type | Gray matter disease, failure to thrive | |
| Tay-Sachs disease | Seizures, cherry red macula, edema, coarse facies | |
| Zellweger syndrome | Hypotonia, high forehead, flat facies | |
| Gaucher disease (neuronopathic form) | Extensor posturing, irritability | |
| Carbohydrate-deficient glycoprotein syndromes | Dysmyelination, cerebellar hypoplasia | |
| <2, without hepatomegaly | Krabbe disease | Irritability, extensor posturing, optic atrophy and blindness |
| Rett syndrome | Girls with deceleration of head growth, loss of hand skills, hand wringing, impaired language skills, gait apraxia | |
| Maple syrup urine disease | Poor feeding, tremors, myoclonus, opisthotonos | |
| Phenylketonuria | Light pigmentation, eczema, seizures | |
| Menkes kinky hair disease | Hypertonia, irritability, seizures, abnormal hair | |
| Subacute necrotizing encephalopathy of Leigh | White matter disease | |
| Canavan disease | White matter disease, macrocephaly | |
| Neurodegeneration with brain iron accumulation disease | White matter disease, movement disorder | |
| 2-5 | Niemann-Pick disease types III and IV | Hepatosplenomegaly, gait difficulty |
| Wilson disease | Liver disease, Kayser-Fleischer ring; deterioration of cognition is late | |
| Gangliosidosis type II | Gray matter disease | |
| Neuronal ceroid lipofuscinosis | Gray matter disease | |
| Mitochondrial encephalopathies (e.g., myoclonic epilepsy with ragged red fibers [MERRF]) | Gray matter disease | |
| Ataxia-telangiectasia | Basal ganglia disease | |
| Huntington disease (chorea) | Basal ganglia disease | |
| Neurodegeneration with brain iron accumulation syndrome | Basal ganglia disease | |
| Metachromatic leukodystrophy | White matter disease | |
| Adrenoleukodystrophy | White matter disease, behavior problems, deteriorating school performance, quadriparesis | |
| 5-15 | Adrenoleukodystrophy | Same as for adrenoleukodystrophy in 2 to 5 yr olds |
| Multiple sclerosis | White matter disease | |
| Neuronal ceroid lipofuscinosis, juvenile and adult (Spielmeyer-Vogt and Kufs disease) | Gray matter disease | |
| Schilder disease | White matter disease, focal neurologic symptoms | |
| Refsum disease | Peripheral neuropathy, ataxia, retinitis pigmentosa | |
| Sialidosis II, juvenile form | Cherry red macula, myoclonus, ataxia, coarse facies | |
| Subacute sclerosing panencephalitis | Diffuse encephalopathy, myoclonus; may occur years after measles |
From Kliegman RM, Greenbaum LA, Lye PS: Practical strategies in pediatric diagnosis and therapy, ed 2, Philadelphia, 2004, Elsevier/Saunders, p 542.
592.1 Sphingolipidoses
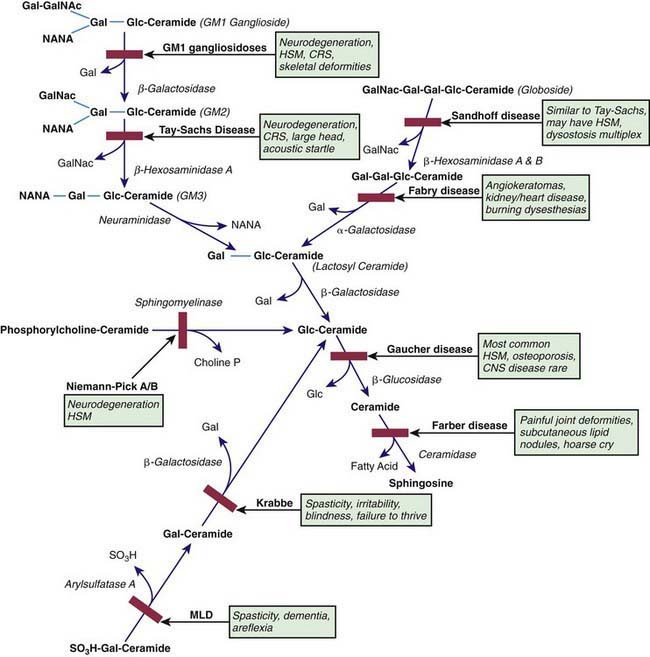
The sphingolipidoses are characterized by intracellular storage of lipid substrates resulting from defective catabolism of the sphingolipids comprising cellular membranes (Fig. 592-1). The sphingolipidoses are subclassified into 6 categories: Niemann-Pick disease, Gaucher disease, GM1 gangliosidosis, GM2 gangliosidosis, Krabbe disease, and metachromatic leukodystrophy. Niemann-Pick disease and Gaucher disease are discussed in Chapter 80.4.
Gangliosidoses (Chapter 80.4)
GM1 Gangliosidoses
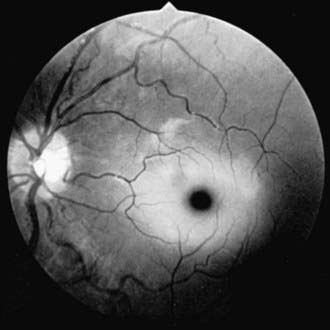
Infantile GM1 gangliosidosis presents at birth or during the neonatal period with anorexia, poor sucking, and inadequate weight gain. Development is globally retarded, and generalized seizures are prominent. The phenotype is striking and shares many characteristics with Hurler syndrome. The facial features are coarse, the forehead is prominent, the nasal bridge is depressed, the tongue is large (macroglossia), and the gums are hypertrophied. Hepatosplenomegaly is present early in the course as a result of accumulation of foamy histiocytes, and kyphoscoliosis is evident because of anterior beaking of the vertebral bodies. The neurologic examination is dominated by apathy, progressive blindness, deafness, spastic quadriplegia, and decerebrate rigidity. A cherry red spot in the macular region is visualized in approximately 50% of cases. The cherry red spot is characterized by an opaque ring (sphingolipid-laden retinal ganglion cells) encircling the normal red fovea (Fig. 592-2). Children rarely survive beyond age 2-3 yr, and death is due to aspiration pneumonia.
GM2 Gangliosidoses
The GM2 gangliosidoses are a heterogeneous group of autosomal recessive inherited disorders that consist of several subtypes, including Tay-Sachs disease (TSD), Sandhoff disease, juvenile GM2 gangliosidosis, and adult GM2 gangliosidosis. Tay-Sachs disease is most prevalent in the Ashkenazi Jewish population and has an approximate carrier rate of 1/30. TSD is due to mutations in the HEXA gene located on chromosome 15q23-q24. Affected infants appear normal until ≈6 mo of age, except for a marked startle reaction to noise that is evident soon after birth. Affected children then begin to lag in developmental milestones and, by 1 yr of age, they lose the ability to stand, sit, and vocalize. Early hypotonia develops into progressive spasticity, and relentless deterioration follows, with convulsions, blindness, deafness, and cherry red spots in almost all patients (see Fig. 592-2). Macrocephaly becomes apparent by 1 yr of age and results from the 200- to 300-fold normal content of GM2 ganglioside deposited in the brain. Few children live beyond 3-4 yr of age, and death is usually associated with aspiration or bronchopneumonia. A deficiency of the isoenzyme hexosaminidase A is found in tissues of patients with TSD. Mass screening for prenatal diagnosis of TSD is a reliable and cost-effective method of prevention because the condition occurs most frequently in a defined population (Ashkenazi Jews). Targeted screening is responsible for the fact that currently, the rare children with TSD born in the USA are most commonly born to non-Jewish parents who are not routinely screened. An accurate and inexpensive carrier detection test is available (serum or leukocyte hexosaminidase A), and the disease can be reliably diagnosed by chorionic villus sampling in the 1st trimester of pregnancy in couples at risk (heterozygote parents).



