Neonatal Seizures
Edward J. Novotny Jr.
Seizures have long been known to be an important sign of neurologic disease in the newborn and accompany neonatal encephalopathies due to a variety of causes. Recent evidence has raised concerns that both seizures and certain medications used in their treatment result in increased risk of neurologic mortality and morbidity. Over the last two decades, bedside video/electroencephalogram (EEG)/polygraphic monitoring in neonates with suspected seizures has raised some important issues regarding the clinical diagnosis of seizures. Two important points have been demonstrated by these studies. First, a significant number of clinical phenomena thought to represent seizures have no accompanying EEG changes on surface recordings. Second, many seizures diagnosed by electroencephalographic criteria have no associated clinical features. This information suggests both that certain types of neonatal seizures may have been overestimated and that the total number of seizures may have been underestimated in the past. These new findings present a diagnostic and therapeutic challenge to clinicians caring for these children and have resulted in recent changes in the classification, diagnosis, and therapy of seizures in the newborn.
CLASSIFICATION AND CLINICAL MANIFESTATIONS
Neonatal seizures are common and occur in 0.5% to 3.5% of newborns, with a slightly higher incidence in preterm infants. Inconsistency in epidemiologic data is the result of variability in the diagnostic criteria and the populations being studied. The classification is best achieved by distinguishing those infants with primary motor features such as tonic, clonic, and myoclonic activity versus subtle clinical seizure types (Box 36.1).
Generalized tonic–clonic seizures are very rare in the newborn. The behavioral phenomena that most consistently correlate with EEG seizure discharges are partial motor and myoclonic seizures. Clonic seizures involving one limb, one side of
the body, and axial structures such as the tongue and face reliably have accompanying synchronous EEG discharges. These clonic movements are rhythmic and occur at a slow rate of one to four times per second. A feature more commonly observed in neonates is that the clonic activity is multifocal or migratory. This characteristic may cause the seizures to appear generalized. The EEG discharges typically consist of runs of rhythmic sharp–slow wave complexes that spread ipsilaterally over the hemisphere from which they originate. Often the clonic activity is not observed until the EEG discharges spread to the central regions near the motor cortex. At this time the motor activity is synchronized with the EEG activity. Focal tonic seizures in which the infant has sustained deviation of the eyes with or without head deviation and asymmetric posturing of the limbs or trunk are frequently associated with electrographic seizures. The EEG discharges associated with tonic seizures involving the limbs usually consist of rhythmic, high-frequency sharp waves and spikes arising from the frontotemporal regions. The eye deviation is associated with similar discharges arising from the occipital scalp electrodes. Generalized myoclonic seizures are another type, which often have associated electrocortical discharges. The myoclonus occurs sporadically or in a few slow series of jerks. The EEG typically shows high amplitude spike-, sharp-, and slow-wave transients synchronized with the motor activity.
the body, and axial structures such as the tongue and face reliably have accompanying synchronous EEG discharges. These clonic movements are rhythmic and occur at a slow rate of one to four times per second. A feature more commonly observed in neonates is that the clonic activity is multifocal or migratory. This characteristic may cause the seizures to appear generalized. The EEG discharges typically consist of runs of rhythmic sharp–slow wave complexes that spread ipsilaterally over the hemisphere from which they originate. Often the clonic activity is not observed until the EEG discharges spread to the central regions near the motor cortex. At this time the motor activity is synchronized with the EEG activity. Focal tonic seizures in which the infant has sustained deviation of the eyes with or without head deviation and asymmetric posturing of the limbs or trunk are frequently associated with electrographic seizures. The EEG discharges associated with tonic seizures involving the limbs usually consist of rhythmic, high-frequency sharp waves and spikes arising from the frontotemporal regions. The eye deviation is associated with similar discharges arising from the occipital scalp electrodes. Generalized myoclonic seizures are another type, which often have associated electrocortical discharges. The myoclonus occurs sporadically or in a few slow series of jerks. The EEG typically shows high amplitude spike-, sharp-, and slow-wave transients synchronized with the motor activity.
BOX 36.1 Clinical Classification of Neonatal Seizures
Tonic
Focal
Generalized
Clonic
Focal
Hemiconvulsive
Myoclonic
Focal
Generalized
Complex motor automatisms
Oromotor—tongue, mouth
Oculomotor—nystagmus, eye deviation
Progressive movements—swimming, bicycling
Miscellaneous
Autonomic—apnea (rarely a seizure when only feature), cardiac arrhythmias, blood pressure changes
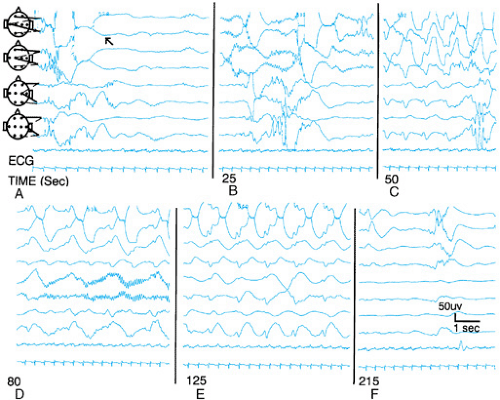 FIGURE 36.1. Subclinical electrographic seizure in a 2-day-old, 29-week estimated gestational age neonate with severe perinatal asphyxia and bilateral intraventricular hemorrhages. The seizure begins with low-amplitude rhythmic alpha activity in the left temporal region (arrow). This builds up in amplitude and spreads to the left central region 25 seconds into the ictal event. Fifty seconds into the seizure irregular, sharp–slow waves are observed over the entire left hemisphere, are higher amplitude anteriorly, and spread to the right frontal region. Rhythmic alpha activity is observed to arise from the right central region 80 seconds into the seizure when the infant was noted to open the left eye. The sharp–slow wave activity is maximum over the left temporal region with spread over the entire cortex 125 seconds into the seizure, which ends 215 seconds from its inception. |
The behavioral phenomena that have a variable association with EEG seizure discharges are the generalized tonic, irregular myoclonic, and subtle neonatal seizures. This last category is also referred to as motor automatism, and specific types may have a greater association with electrographic seizures depending on other clinical features. The subtle neonatal seizure that is the most commonly observed type in several studies has a poor association with EEG seizure discharges in the full-term neonate. However, there is a greater association with electrographic seizures in the premature infant. Their clinical features may further divide subtle seizures into those involving the mouth and tongue, the eyes, and more complex movements such as pedaling, swimming, and stepping. The premature neonates often have simple subtle seizures with eye, mouth, and tongue movements. The electrographic seizures in the premature infants are very distinctive and have a characteristic progression and spread throughout multiple cortical regions with minimal accompanying clinical signs (Fig. 36.1). In the term infant who has more complex motor automatisms, there is often no associated EEG discharge. Myoclonic activity that is irregular, multifocal, and often stimulus-induced is typically not associated with any changes in electrocortical activity. These infants usually have markedly abnormal EEGs for gestational age with suppressed and poorly differentiated background. The infants who have episodes described as generalized tonic seizures rarely have them as a result of an epileptic seizure. Less than 15% of infants with these clinical phenomena had electrographic seizures as a cause. These episodes most
probably represent decerebrate and decorticate posturing from acute intracranial pathology.
probably represent decerebrate and decorticate posturing from acute intracranial pathology.
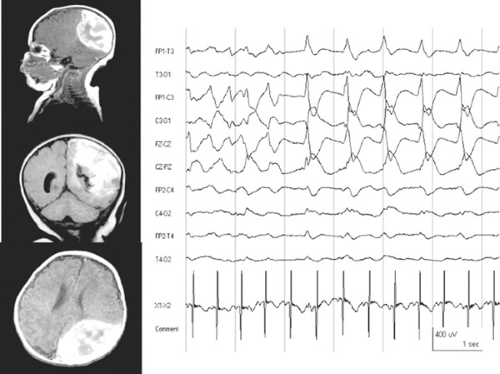 FIGURE 36.2. Magnetic resonance imaging (MRI) scan of the head and electroencephalogram (EEG) of a term infant observed to have clonic activity predominantly involving the right side of the body in the first day of life. The MRI on the left shows sagittal, coronal, and axial T1-weighted images (from top to bottom) demonstrating a large hemorrhagic stroke involving the left parietal lobe. The EEG demonstrates nearly continuous epileptic discharges arising from the left hemisphere and midline scalp electrodes. The odd-numbered channels are from the left side of the scalp and even-numbered channels are from the right side. The infant was having nearly continuous right arm and leg motor activity at the time of the EEG. |
Clinical attributes that differentiate clonic seizures from tremors and clonus are that infants with clonic seizures have slower, more rhythmic motor activity that cannot be restrained, whereas infants with tremors and clonus have rapid, irregular motor activity that ceases with restraint and change in posture. Tremor, clonus, and other nonepileptic motor automatisms are typically induced by various tactile, noxious, and auditory stimuli. Nonepileptic phenomena also demonstrate properties of spatial and temporal summation with increased intensity or frequency of the stimulus. These latter behaviors are abnormal and usually indicate the existence of an encephalopathy, but they do not represent behaviors that warrant treatment with antiepileptic therapy. Another clinical characteristic that aids in distinguishing epileptic from nonepileptic abnormal behavioral phenomena is that epileptic seizures are typically accompanied by changes in heart rate, respiratory pattern, pupil size, and blood pressure. Further video/EEG/polygraphic studies are required in the neonate to better define the temporal and spatial relationships of these autonomic changes with the electroclinical seizure.
As suggested by several investigators, the more recent information on both underestimation and overestimation of neonatal seizures and the past lack of a consensus of what phenomena are truly epileptic seizures in the newborn make all previous investigations of etiology, treatment, and prognosis of limited value. These concerns have the greatest impact on treatment, since prognosis and etiology are interdependent and the seizures are simply a symptom of an underlying neuropathologic process. Recent concerns regarding the effects of antiepileptic drug therapy on the developing nervous system has increased the importance of these issues.
ETIOLOGY AND DIAGNOSIS
The causes of neonatal seizures include perinatal asphyxia, central nervous system infections, intracranial hemorrhages, and cerebral infarcts; these are the most common disorders responsible for neonatal seizures. Developmental anomalies, acute metabolic disorders, and rare inborn errors of metabolism are less common causes. The identification of the latter two categories of causes is crucial since the treatment is management of the underlying disease. Certain types of seizures are observed in infants with specific disorders. Persistent partial motor seizures are typically observed in infants with strokes (Fig. 36.2). Clonic seizures are also commonly seen in infants with hypocalcemia, the incidence of which has decreased dramatically in recent decades. Subtle and tonic seizures are more common in infants with hypoxic-ischemic encephalopathy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


