Neonatal Proximal Bowel Obstruction
Steven J. Kraus, MD
DIFFERENTIAL DIAGNOSIS
Common
Esophageal Atresia (EA)
Duodenal Atresia (DA) or Stenosis (DS)
Duodenal Web (DW)
Jejunal Atresia
Less Common
Hiatal Hernia
Midgut Volvulus (MV)
Annular Pancreas
Preduodenal Portal Vein
Rare but Important
Gastric Atresia
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Many neonates diagnosed prenatally by US or MR
Inability to pass nasogastric tube suggests EA
Neonate usually has difficulty swallowing secretions
Look for other radiologic findings of VATER or VACTERL
Vertebral anomalies, anorectal malformation, renal anomalies, radial ray anomalies, congenital heart defects
Radiographs can be diagnostic for duodenal atresia
“Double bubble” (rounded duodenum)
Air-filled duodenum without complete distention → immediate upper GI to exclude MV (surgical emergency)
Look for signs of Down syndrome
11 rib pairs
Cardiomegaly, shunt physiology
Duodenal dilation with distal gas in face of bilious emesis is suspicious for midgut volvulus
Immediate upper GI required
Radiographs show “triple bubble” of jejunal atresia
Contrast enema sometimes to assess for distal atresia (suggested by microcolon)
Radiograph showing retrocardiac lucency suggests hiatal hernia
UGI can confirm
Frequently associated with gastric volvulus
Annular pancreas almost always associated with DA
Preduodenal portal vein rarely found in isolation
Gastric atresia usually with other atresias, not isolated
Helpful Clues for Common Diagnoses
Esophageal Atresia (EA)
Intermittent fluid distention of proximal esophagus on fetal imaging
High T2 signal in distended pouch on fetal MR
Anechoic fluid distention of pouch on fetal US
Air-filled esophageal pouch on newborn chest radiograph
Nasogastric tube tip upper esophagus
Sometimes associated tracheoesophageal fistula (TEF); preoperative esophagram
Lateral position esophagram to show fistula
Fistula usually just above carina; extends anterior and superior toward trachea
Sometimes associated with laryngotracheal cleft
Faulty division of foregut
50-75% have associated anomalies
5 types
Proximal EA with distal TEF (82%)
EA without TEF (10%)
Isolated TEF (H type) (4%)
EA with proximal and distal TEF (2%)
EA with proximal TEF (2%)
Duodenal Atresia (DA) or Stenosis (DS)
Dilated, round proximal duodenum and stomach “double bubble” on fetal imaging
Anechoic, high T2 signal in round D1-2 segment on fetal US/MR
Air-filled “double bubble”; no distal gas on neonatal radiograph
If duodenum initially not rounded (partially distended), cannot exclude MV; immediate upper GI indicated
Most common upper bowel obstruction in neonate
Failure of vacuolization (recanalization) during embryogenesis
Up to 33% also have annular pancreas
Up to 33% also have Down syndrome
Up to 28% also have malrotation
Jejunal Atresia
“Triple bubble” on neonatal radiographs
Dilated air-filled stomach, duodenum, and proximal jejunum without distal gas
No other imaging generally required
Microcolon on water-soluble enema suggests additional distal atresia
Dilated fluid-filled proximal bowel loops on fetal sonography or MR
Absence or complete occlusion of intestinal lumen of segment of jejunum
Likely due to in utero ischemic event
Helpful Clues for Less Common Diagnoses
Hiatal Hernia
Neonatal radiography shows retrocardiac density overlying mid to right heart
Upper GI shows gastroesophageal junction and stomach above diaphragm
Sliding hiatal hernia does not usually cause bowel obstruction
Traction or torsion (volvulus) of stomach is common
Can be associated with congenital short esophagus
Midgut Volvulus (MV)
Abnormal twisting of small bowel around superior mesenteric artery causing obstruction ± bowel ischemia/necrosis
Most frequent finding on abdominal radiography is normal bowel pattern
Multiple dilated bowel loops is later finding, likely due to ischemic ileus
Late findings: Pneumatosis, portal venous gas, gasless abdomen, free intraperitoneal air
UGI
Duodenal dilation to 2nd segment of duodenum
Cone-shaped appearance of D2 segment with decompressed D3 and distal bowel
Usually duodenojejunal junction (DJJ) low and not at, or to left of, left vertebral pedicle on AP image (malrotation)
Rare cases of MV with normal duodenal rotation
Corkscrew appearance of duodenum and proximal jejunum
If contrast obstructed at D2, cannot exclude MV; may indicate surgical exploration at surgeon’s discretion
If enema performed, may show nonrotation with spiral course of colon involved in volvulus
Annular Pancreas
Similar radiographic and UGI findings as DA, DW, MV
Band of pancreatic tissue surrounds D2
Preduodenal Portal Vein
Radiographic and UGI findings similar to DA, DW, MV
Helpful Clues for Rare Diagnoses
Gastric Atresia
No gas beyond stomach; UGI: Gastric outlet obstruction
Usually with multiple intestinal atresias
Enema: Usually microcolon due to distal atresias
Image Gallery
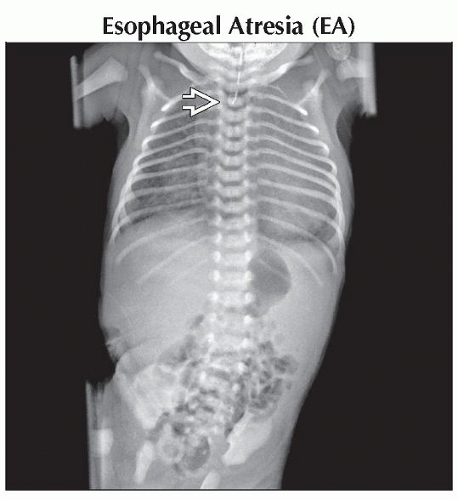 AP radiograph shows feeding tube tip overlying thoracic inlet  due to EA. The abdominal gas indicates a TEF. Ribs are gracile. No vertebral anomalies. Question congenital heart disease. due to EA. The abdominal gas indicates a TEF. Ribs are gracile. No vertebral anomalies. Question congenital heart disease. |
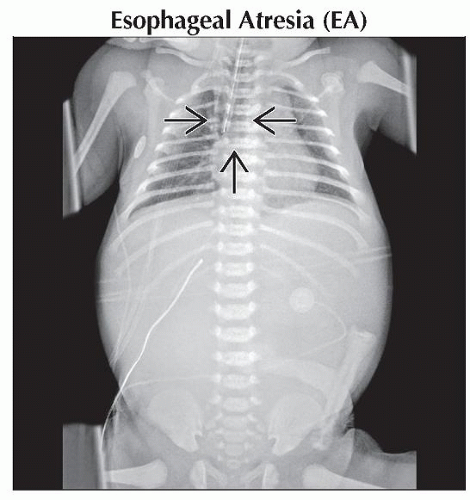 AP radiograph of the chest/abdomen in another patient shows EA pouch  without fistula; there is no gas beyond atretic esophagus. without fistula; there is no gas beyond atretic esophagus. |
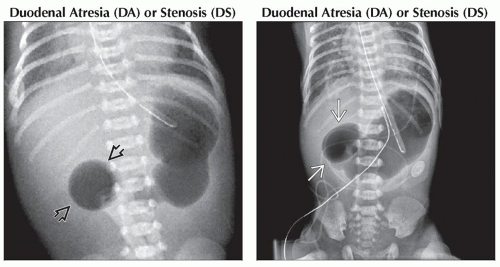 (Left) Anteroposterior radiograph of a newborn shows a dilated, air-filled stomach and dilated, spherical proximal duodenum
 with no distal gas, consistent with DA. The presence of cardiomegaly, pulmonary edema, and 11 rib pairs suggests Down syndrome. (Right) Anteroposterior radiograph shows a “double bubble” sign of duodenal atresia: Dilated, air-filled stomach and round, obstructed proximal duodenum with no distal gas, consistent with DA. The presence of cardiomegaly, pulmonary edema, and 11 rib pairs suggests Down syndrome. (Right) Anteroposterior radiograph shows a “double bubble” sign of duodenal atresia: Dilated, air-filled stomach and round, obstructed proximal duodenum  . .Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|