Middle Mediastinal Mass
Eric J. Crotty, MD
DIFFERENTIAL DIAGNOSIS
Common
Lymphoma
Bronchogenic Cyst
Less Common
Lymphadenopathy
Vascular Anomalies
Rare but Important
Postoperative Complications
Pericardial Lesions
Malignant Tumors
ESSENTIAL INFORMATION
Helpful Clues for Common Diagnoses
Lymphoma
Usually occurs with confluent multicompartment disease that involves anterior mediastinum
Most commonly involves paratracheal > hilar > subcarinal groups
Homogeneous or heterogeneous soft tissue attenuation and signal intensity on CT and MR
May compress or invade superior vena cava (SVC), esophagus, tracheobronchial tree, and pericardium
SVC more often compressed without associated obstruction, but invasion may lead to SVC syndrome
Bronchial involvement may lead to lobar collapse
Pericardial involvement can result in pericardial effusion
Bronchogenic Cyst
May have bronchial or esophageal origin
Most commonly paratracheal or subcarinal
Collapse or hyperlucency may occur as result of bronchial compression
Usually round or oval with smooth contour
Homogeneous density on radiograph and attenuation on CT
Classically fluid attenuation but may be of higher attenuation due to high protein content
Wall of cyst is thin and does not enhance unless complicated by infection
Variable low T1 and homogeneously increased T2 signal on MR
Characteristically thin and nonenhancing wall unless infected
Helpful Clues for Less Common Diagnoses
Lymphadenopathy
Usually related to infection in pediatric population
Most common inciting organism depends on geographic location
Consider primary tuberculosis (TB), histoplasmosis, coccidioidomycosis, and blastomycosis
TB and histoplasmosis may have lymph nodes with low-attenuation centers on contrast-enhanced CT in acute phase
Calcification of lymph nodes indicates more remote disease
Vascular Anomalies
Most commonly due to congenital anomalies of aorta and its branches
Findings are more apparent on positive contrast studies of esophagus
Anomalous vessels are most easily seen on CT and MR
Convexity to right of trachea on radiograph may be due to right aortic arch or double aortic arch
Posterior impression/anterior bowing of trachea on lateral radiograph may be due to
Diverticulum of Kommerell related to aberrant subclavian artery
Passage of aorta across midline posterior to trachea and esophagus
Dilatation of ascending aorta
Seen in congenital aortic valvar or supravalvar stenosis (Turner syndrome and Williams syndrome)
Also may be seen in connective tissue disorders (Ehlers-Danlos and Marfan syndrome)
Convexity along right mediastinal border on chest radiograph
Dilatation of ascending aorta best seen on CT and MR
Pulmonary arterial lesions are less common
Anomalous origin of left pulmonary artery from right pulmonary artery (pulmonary arterial sling)
Left pulmonary artery passes between trachea and esophagus
Passage of LPA between trachea and esophagus is best appreciated on CT and MR but also well seen on positive contrast studies of esophagus
Pulmonic valve stenosis may lead to poststenotic dilatation of main pulmonary arterial segment
Convexity in aortopulmonary window on radiography
Seen as dilatation of MPA on CT and MR
May also involve azygous vein and anomalous pulmonary venous drainage
Azygous vein enlargement leads to convexity above right main bronchus
Most commonly related to azygous continuation of IVC
May also be secondary to obstruction of SVC
Supracardiac type of anomalous pulmonary venous return leads to “snowman” appearance of mediastinum on radiograph
Helpful Clues for Rare Diagnoses
Postoperative Complications
Some fluid always present in operative bed following cardiac surgery
Usually resolves in early days following surgery with gradual decrease in size of mediastinum
Concern if radiograph demonstrates increased widening of mediastinum
May be hematoma, seroma, or infection
Hematoma may be associated with pseudoaneurysm at surgical site
Contrast protrusion from vessel lumen on CT with signal changes of denatured blood and flow void on MR
Pericardial Lesions
Pericardial effusion is seen as enlargement of cardiac silhouette with “water bottle” configuration on radiography
Lungs usually clear
“Fat pad” sign on lateral chest radiograph is rarely seen due to relative lack of fat in mediastinum in pediatric population
May be secondary to infection (most commonly viruses), following surgery or trauma, or related to neoplasia (lymphoma)
Pericardial cyst consists of various-sized loculations of fluid
Rounded convexity, most commonly in right cardiophrenic angle on radiography
Loculated fluid attenuation and signal on CT and MR respectively
Pericardial tumors are uncommon
Malignant Tumors
Both primary and secondary malignant tumors are very rare, excluding lymphoma
Consider carcinoid, melanoma, rhabdomyosarcoma, malignant germ cell tumors, squamous cell carcinoma in patients with respiratory papillomatosis
Image Gallery
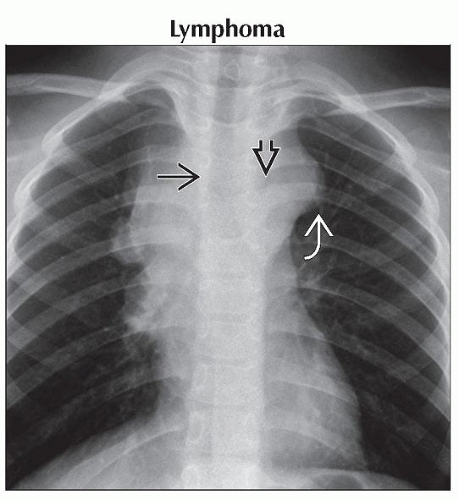 Posteroanterior radiograph shows a lobulated middle mediastinal mass  with loss of the normal thin right paratracheal stripe with loss of the normal thin right paratracheal stripe  and nonvisualization of the outline of the aortic arch and nonvisualization of the outline of the aortic arch  . . |
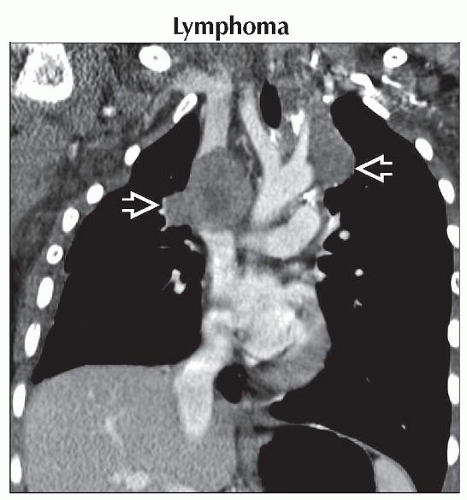 Coronal CECT shows the lobulated contour of the middle mediastinum  due to involvement with lymphoma. Hodgkin and non-Hodgkin lymphoma cannot be differentiated by imaging. due to involvement with lymphoma. Hodgkin and non-Hodgkin lymphoma cannot be differentiated by imaging. |
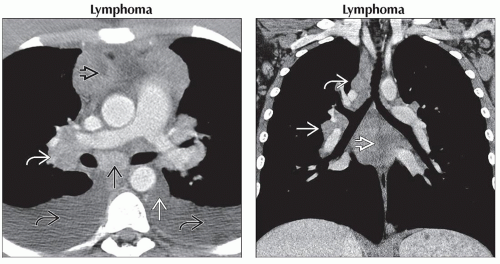 (Left) Axial CECT shows a somewhat heterogeneous mass in the anterior
 , middle , middle  , and posterior , and posterior  mediastinum and in the right hilum mediastinum and in the right hilum  . There are also bilateral pleural effusions . There are also bilateral pleural effusions  . Lymphoma most commonly involves the anterior mediastinum but can involve the other mediastinal compartments. Pleural effusions are common. (Right) Coronal CECT shows the tumor involving the subcarinal . Lymphoma most commonly involves the anterior mediastinum but can involve the other mediastinal compartments. Pleural effusions are common. (Right) Coronal CECT shows the tumor involving the subcarinal  , right paratracheal , right paratracheal  , and right hilar , and right hilar  regions. regions.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|