Mediastinal Widening
Alexander J. Towbin, MD
DIFFERENTIAL DIAGNOSIS
Common
Normal Thymus
Lymphoma
Reactive Lymphadenopathy
Less Common
Bronchogenic Cyst
Trauma
Enlargement of Ascending Aorta
Rare but Important
Germ Cell Tumor
Neurofibromatosis Type 1
Thyroid Carcinoma
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Normal pediatric mediastinum is wider than in adulthood due to thymus
Trauma is uncommon cause of mediastinal widening in children
Helpful Clues for Common Diagnoses
Normal Thymus
Most common mediastinal “mass” in neonates and infants
Most prominent in infancy
Has quadrilateral shape
Thymus increases in weight until adolescence when it begins to involute
Gradually becomes triangular-shaped in childhood and teenage years
Visible by radiograph until ˜ 5 years of age
Appearance may change with respiration
Thymus can vary in size depending on intercurrent illness and stress
May ↓ in size during illness/stress and → in size with recovery
Often asymmetric across midline
Usually more prominent on right side
Mimic upper lobe consolidation
Homogeneous appearance on CT and MR
Enhances homogeneously
Multiple linear echoes and discrete echogenic foci on ultrasound
Lymphoma
3rd most common malignancy in children after leukemia and brain tumors
Incidence increases with age
25% of cancers in children 15-19 yo
Most common mediastinal mass in teens
Hodgkin lymphoma (HL) more common than non-Hodgkin lymphoma (NHL)
HL involves continuous nodal groups
NHL is more commonly extranodal
NHL is more common than HL in children < 10 years of age
Mediastinal disease is common in HL and NHL
Occurs in 2/3 with HL
Mediastinal mass can cause tracheal compression
Reactive Lymphadenopathy
Most common organism depends on geographic location
Common causes: Tuberculosis (TB), histoplasmosis, coccidioidomycosis, and blastomycosis
TB and histoplasmosis may have lymph nodes with low-attenuation centers on contrast-enhanced CT in acute phase
Lymph node calcification in old disease
Enlarged lymph nodes can compress superior vena cava (SVC)
May cause SVC syndrome or fibrosing mediastinitis
Helpful Clues for Less Common Diagnoses
Bronchogenic Cyst
May have bronchial or esophageal origin
Most common location: Paratracheal or subcarinal
May lead to bronchial compression
May cause atelectasis or hyperinflation
Round or oval with smooth contour
Homogeneous appearance
Typically fluid attenuation on CT
Can have higher density with ↑ protein content, hemorrhage, or infection
Wall of cyst is thin and does not enhance unless complicated by infection
Variable low T1 and homogeneously increased T2 signal on MR
Characteristically thin and nonenhancing wall unless infected
Trauma
Most common cause of death in children
Mediastinal hematoma is cause of mediastinal widening in trauma
Traumatic aortic injuries are uncommon
Iatrogenic trauma is most common cause of aortic injury in children
Aortic injury most common in teens
Associated traumatic injuries are common
Enlargement of Ascending Aorta
Aortic valve stenosis
Results in poststenotic dilatation
Can be valvular, subaortic, or supravalvular
Valvular aortic stenosis is most common
Can be seen in Turner syndrome and is associated with bicuspid aortic valve and coarctation of aorta
Supravalvar aortic stenosis is seen in Williams syndrome
Dilated aorta often caused by aneurysm
Causes of aortic aneurysm: Connective tissue disorders, vasculitis, trauma, or infection
Connective tissue disorders: Marfan syndrome, Ehlers-Danlos, Loeys-Dietz
Marfan and Ehlers-Danlos are disorders of collagen synthesis
Dilatation of sinus of Valsalva and ascending aorta
Other systemic manifestations
Vasculitis: Takayasu arteritis
Large vessel vasculitis
Affects aorta, its main branches, and pulmonary arteries
Mycotic aneurysm
Uncommon in children
Can occur in infants secondary to umbilical arterial line
Helpful Clues for Rare Diagnoses
Germ Cell Tumor
Originate from germ cells that fail to complete migration from urogenital ridge
Mediastinum is 4th most common site for teratoma (ovary, sacrococcygeal, testis)
Often contain tissues that derive from germinal cell layers
Can be cystic
Neurofibromatosis Type 1
Autosomal dominant disorder
Classical clinical findings of café au lait spots, axillary freckling, and dermal and plexiform neurofibromas
Plexiform neurofibromas can occur anywhere
Plexiform neurofibromas have targetoid appearance on MR
Loss of targetoid appearance should raise concern for degeneration into malignant peripheral nerve sheath tumor
Thyroid Carcinoma
Uncommon in children
Most common pediatric endocrine tumor
Thyroid nodules seen in up to 1.5%
Nodules > 1 cm should be biopsied
Radiation exposure is risk factor
Image Gallery
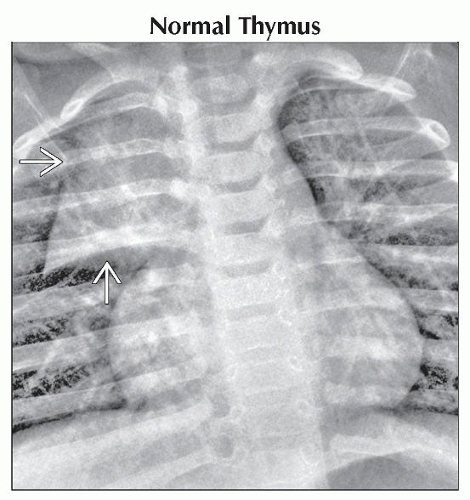 PA radiograph of the chest shows a sail-like appearance of the normal thymus  . The lateral border of the thymus typically has an undulating contour along the anterior lateral chest wall. . The lateral border of the thymus typically has an undulating contour along the anterior lateral chest wall. |
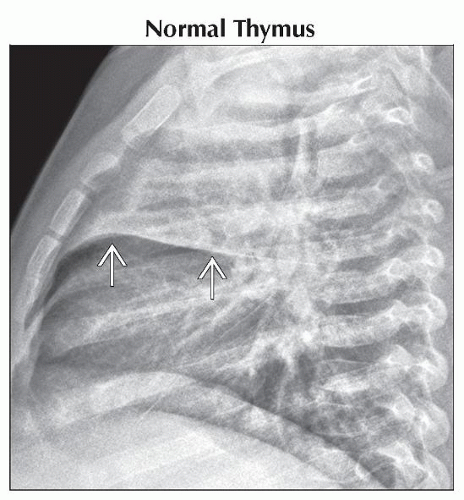 Lateral radiograph of the chest in the same patient shows the thymus in the anterior mediastinum filling in the retrosternal clear space  . This is a typical finding in young children. . This is a typical finding in young children. |
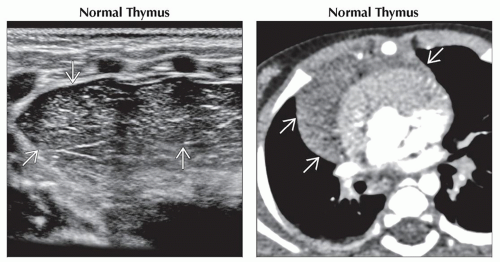 (Left) Longitudinal ultrasound shows the normal thymus
 just below the anterior chest wall. On ultrasound, the thymus has multiple linear echoes and discrete echogenic foci. Ultrasound is useful to distinguish a normal thymus from a mediastinal mass. (Right) Axial CECT shows the normal thymus just below the anterior chest wall. On ultrasound, the thymus has multiple linear echoes and discrete echogenic foci. Ultrasound is useful to distinguish a normal thymus from a mediastinal mass. (Right) Axial CECT shows the normal thymus  draped over the superior aspect of the heart. On CT, the thymus has a homogeneous soft tissue density with homogeneous enhancement. draped over the superior aspect of the heart. On CT, the thymus has a homogeneous soft tissue density with homogeneous enhancement.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|