Meckel Diverticulum
Wilhelm Fabricius Hildanus, a German surgeon, first described the presence of a small bowel diverticulum in 1598.1 However, the diverticulum is named for Johann Meckel, a German anatomist, who further described the anatomy and embryology in 1809.2 Meckel diverticulum is a remnant of the embryologic vitelline (omphalomesenteric) duct that connects the fetal gut with the yolk sac and normally involutes between the fifth and seventh weeks of gestation. Failure of duct regression results in a variety of abnormalities arising from persistence of the remnant (Fig. 40-1). The most common anomaly (90%) is the classic Meckel diverticulum. It is a true diverticulum, consisting of all normal layers of the bowel wall. Clinical symptoms and complications can arise from small bowel obstruction, bleeding, inflammation, umbilical abnormalities, or neoplasia.
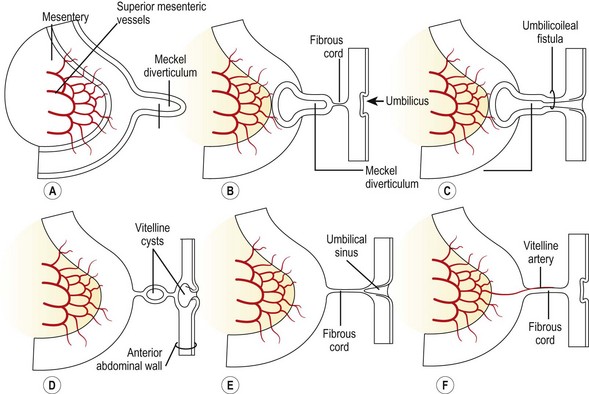
FIGURE 40-1 Drawings illustrating Meckel diverticulum and other remnants of the yolk sac. (From Moore KL. The Developing Human. Philadelphia: WB Saunders; 1988.)
Epidemiology
The true incidence of Meckel diverticulum is unknown, since most patients are asymptomatic. While the incidence is typically estimated at approximately 2%, a recent systematic review of autopsy studies found an incidence of 1.2%.3 The incidence may be increased in patients with major anomalies of the umbilicus, alimentary tract, nervous system, or cardiovascular system.4 An estimated 4% of patients with Meckel diverticulum will become symptomatic, and the risk of developing symptoms decreases with age.5 A recent report based on data from the Pediatric Health Information System database found that 53% of Meckel diverticulectomies are performed before 4 years of age, with a male : female ratio of 2.3 : 1 overall and 3 : 1 in symptomatic patients.6 The commonly cited ‘rule of 2s’ regarding the diverticulum is: occurs in 2% of the population, has a 2 : 1 male : female ratio, usually discovered by 2 years of age, located 2 feet (60 cm) from the ileocecal valve, commonly 2 cm in diameter and 2 inches (5 cm) long, and can contain two types of heterotopic mucosa.7 Gastric is the most common type of heterotopic mucosa, followed by pancreatic (Fig. 40-2).8 More rarely, it may contain duodenal, colonic, or endometrial tissue.
Clinical Presentation
A variety of symptoms can develop depending on the configuration of the remnant structure and the presence of ectopic mucosa. The three most common presentations in children are intestinal bleeding (30–56%), intestinal obstruction (14–42%), and diverticular inflammation (6–14%).8–10 Other less common signs include a cystic abdominal mass11 and a newborn with an umbilical fistula resulting from a patent vitelline duct (Fig. 40-3). A Littré hernia refers to a Meckel diverticulum found incarcerated in a hernia which may be located at the inguinal, femoral, umbilical or Spigelian sites.12 In adults, especially the elderly, neoplasia can develop within the Meckel diverticulum. Carcinoid is the most common tumor, but other malignancies include adenocarcinoma, leiomyosarcoma, gastrointestinal stromal tumors, and lymphoma.13 Neonatal presentation of a Meckel diverticulum is uncommon and typically is due to perforation or obstruction.14
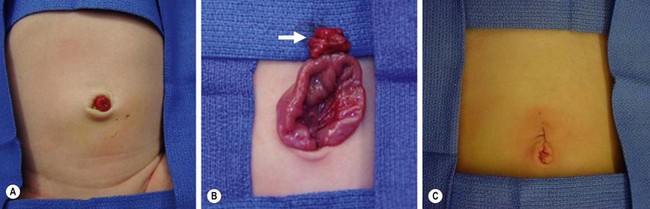
FIGURE 40-3 This neonate was born with an obvious patent omphalomesenteric duct. (A) Meconium was seen to emanate from the stoma. (B) A circumumbilical incision was made, and the duct (arrow) was dissected to its connection with the ileum. (C) The duct was amputated from the ileum and the umbilical incision closed. The patient recovered uneventfully and has not developed any further problems.
Bleeding
Bleeding is generally attributed to the presence of heterotopic mucosa. Gastric mucosa is present in up to 80% of Meckel diverticula that bleed.15 Gastric acid produces mucosal ulceration, typically at the junction of the ectopic mucosa and the normal ileal mucosa. The ulcer may also be located within the ectopic mucosa or even on the mesenteric side of the normal ileum, opposite the diverticulum. While Helicobacter pylori is associated with many ulcers in the duodenum and stomach, studies have shown that H. pylori is rarely present in a bleeding Meckel diverticulum.16,17
Obstruction
A Meckel diverticulum can cause intestinal obstruction through several mechanisms, but most commonly intussusception or volvulus. The diverticulum can act as a lead point for an obstructing ileo-ileal and subsequent ileo-colic intussusception. A volvulus can occur if bowel twists or kinks around a vitelline remnant with a fibrous cord between the diverticula and umbilicus (see Fig. 40-1). An internal hernia can result due to a mesodiverticular artery, coursing from the base of the mesentery to the diverticulum, under which the small bowel becomes entrapped and incarcerated. Other rare obstructing mechanisms include an incarcerated Littré hernia, and a long diverticulum that may knot on itself or twist around its base.



