Marsupialization of Bartholin Gland Cyst
M. Jonathon Solnik
INTRODUCTION
The Bartholin glands are bilateral glands located in the vulva, normally less than 1 cm in diameter, and secrete mucous to provide for vaginal lubrication. The Bartholin ducts, normally lined with transitional epithelium, open into the inner aspect of the introitus. A Bartholin gland may expand and dilate if the gland’s duct becomes obstructed, most commonly after traumatic injury, or even after surgical repair of the posterior vaginal compartment; it occurs less commonly after gonococcal infection. Management of women presenting with symptomatic Bartholin gland cyst obstruction typically depends on whether the obstruction of the duct is acute and associated with inflammation and/or abscess, or whether it is chronic and noninfected. Many women are not symptomatic and may not be aware of such a cyst until noted on gynecologic examination.
A noninfected cyst normally ranges in size from 1 to 3 cm, does not cause pain, and may slowly regress and re-expand over time (Figure 9.1). Alternatively, if it becomes infected, a Bartholin gland cyst can form an abscess that will rapidly increase in size over several days and is very painful. In order to heal, a Bartholin gland cyst abscess usually must be drained. Acute infection, resulting in a painful, pus-filled gland, should be treated by incision and drainage (I & D) and placement of a Word catheter. Irrigation of the gland with sterile saline and manual disruption of any loculations within with a small curved clamp typically results in symptomatic relief. Use of antibiotic irrigant or post-procedural antibiotics have not been shown to be of additional benefit. Cultures, unless suspected for methicillin-resistant Staphylococcus aureus, are not clinically useful. Simple I & D, without the placement of a Word catheter, should be avoided since this does not allow for ongoing drainage, predisposing to recurrence.
Either marsupialization or gland excision, representing more aggressive treatment of a Bartholin gland cyst, are indicated for chronic gland cysts that are symptomatic. Marsupialization should be avoided during the acute phase of infection. Marsupialization, in contrast to gland excision, preserves gland function and may allow for adequate vaginal lubrication after release of the obstruction.
PREOPERATIVE CONSIDERATIONS
Marsupialization is reserved for patients with chronic, symptomatic cysts and avoids complications associated with gland excision, which is more lengthy and morbid. During the preoperative evaluation, a thorough history should be obtained to ascertain risk factors for initial cause, postoperative complications, and potential recurrence. On examination, the size and location of the Bartholin gland should be documented, and the clinician should make certain that the process does indeed involve the Bartholin gland rather than the labia minora or other vaginal glands as the treatment may differ significantly.
Risks of the procedure should be reviewed, including postoperative tenderness, drainage, as well as the need to refrain from coitus for at least 3 to 4 weeks to minimize irritation and trauma. The procedure should
take place in an ambulatory surgery setting since adequate anesthesia (local, regional, moderate sedation) and exposure are needed for marsupialization, as opposed to I & D and Word catheter placement, which can easily be performed in the office setting.
take place in an ambulatory surgery setting since adequate anesthesia (local, regional, moderate sedation) and exposure are needed for marsupialization, as opposed to I & D and Word catheter placement, which can easily be performed in the office setting.
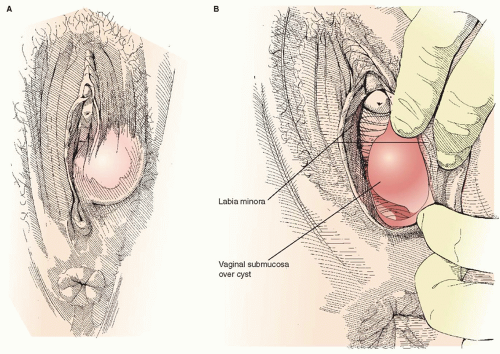 FIGURE 9.1 A left-sided uninfected Bartholin gland cyst (Figure 9.1A
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|