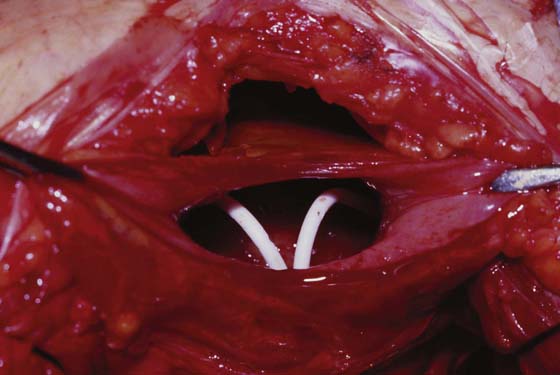
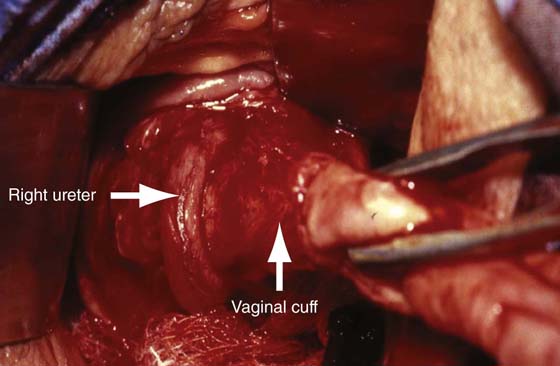
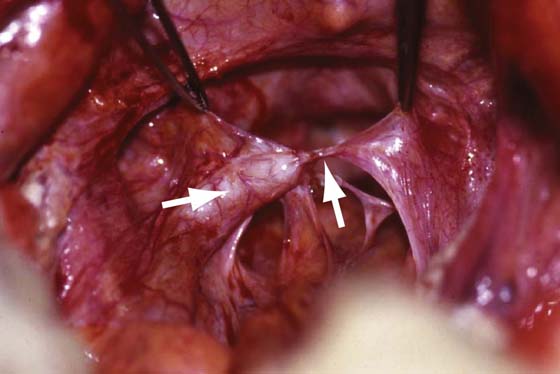
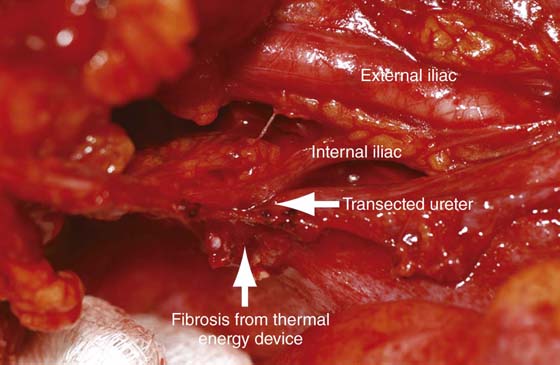
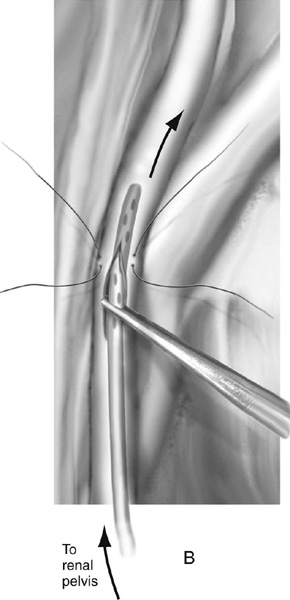
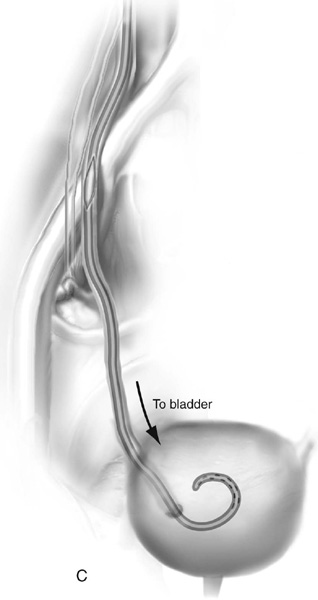
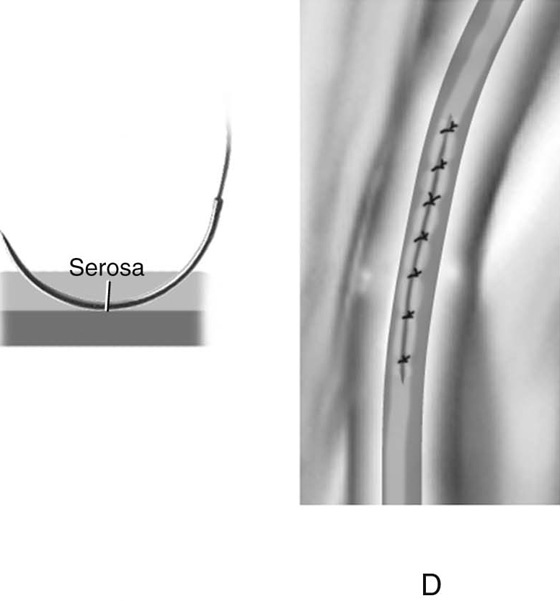
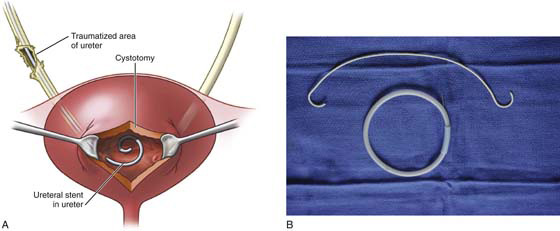
CHAPTER 91 Michael Maggio Injury to the lower urinary tract will occur in approximately 1% to 2% of women undergoing major gynecologic surgery. Although the risk of injury increases with increasing difficulty of the primary operation (e.g., large uterus, excessive bleeding, prolapse procedures, malignancy, endometriosis), more than 50% of injuries occur during uncomplicated procedures. Furthermore, in the absence of cystoscopy, most injuries are undetected during the primary operation, leading to increased morbidity and costs associated with diagnostic procedures, prolonged hospital stay, reoperations, return visits, and delay in diagnosis (e.g., ileus, urosepsis, fistula formation). The incidence of ureteral injury following gynecologic surgery ranges from 0.2% to 11.0%, depending on the type of study (historical vs. prospective) and the definition of injury (kinking from suspension vs. transaction/crush injury). Intraoperative techniques to avoid ureteral injury and the ability to ensure ureteral patency at the time of surgery should be in the realm of every gynecologic surgeon. During vaginal or laparoscopic surgery, cystoscopy after the administration of indigo carmine can be utilized to visualize the spill of blue dye from the ureteral orifices (see section on cystoscopy). During open abdominal surgery, advertent cystotomy with visualization of the ureteral orifices is an option that will avoid repositioning of the patient required for cystoscopy (see Chapter 88). Ureteral catheters can be placed at the time of cystoscopy to help avoid ureteral injury in selected cases (Figs. 91–1 and 91–2). Ureteral anatomy can be variable depending on the anatomy of the patient, as well as the anatomic distortion that can occur when the pelvic abnormality is addressed. Also, overzealous or inappropriate use of an energy source can result in ureteral injury (Figs. 91–3 through 91–5). The surgical procedure utilized to address an intraoperative or postoperative ureteral injury depends on the extent and location of the injury. FIGURE 91–1 A. Schematic representation of a distal right ureteral serosal injury. Injuries of this type can be handled by retrograde stenting of the affected ureter via bladder dome cystotomy. B. 6 French × 26-cm double J stent and wire. The wire is used to make the stent rigid during placement. FIGURE 91–2 Photograph of bladder dome cystotomy with two retrograde placed double J ureteral stents. FIGURE 91–3 Photograph of the right distal ureter entering the bladder (left arrow). The photo illustrates the close proximity of the ureter to the vaginal cuff during a posthysterectomy vault prolapse repair. Failure to identify the ureter before securing the uterosacral and cardinal remnant pedicles (right arrow) would have led to injury. FIGURE 91–4 Photograph of left ureteral obstruction following uterosacral vault suspension. Note the dilated proximal ureter (left arrow) and the offending suture (right arrow). FIGURE 91–5 Photograph of a transected ureter due to inaccurate placement of a thermal energy device at the time of radical hysterectomy. Excessive fibrosis or anatomic distortion of the ureter at times can be encountered intraoperatively. In these situations, it may be beneficial to perform a ureterotomy and pass a stent antegrade into the bladder or retrograde into the kidney. The procedure is performed as follows. Dissection of the ureter should be minimized to prevent ischemic injury by interrupting the blood supply to the ureter and the periureteral tissue. Stay sutures can be placed laterally before the incision is made, and a hook blade can be used for the ureterotomy. The authors prefer a longitudinal incision. The ureter then can be catheterized to ensure patency or determine the level of obstruction, or even to assist in dissection lower down near the bladder. Closure is accomplished with interrupted 4-0 or 5-0 absorbable sutures. Closure should include only the adventitia and superficial incorporation of the ureteral musculature. A double J stent is placed before closure, and a drain is left in place and removed after drainage subsides (Fig. 91–6). FIGURE 91–6 Technique of ureterotomy. A. Stay sutures are placed laterally to facilitate traction on the ureter. A hook blade is used to make a longitudinal incision in the ureter. B. A double J stent is passed antegrade into the kidney and (C) retrograde into the bladder. D. Ureterotomy is closed with interrupted 4-0 or 5-0 absorbable sutures. Closure should include only the adventitia and a superficial incorporation of the ureteral musculature.
Managing Ureteral Injury During Pelvic Surgery
 Emanuel C. Trabuco
Emanuel C. Trabuco  John B. Gebhart
John B. Gebhart
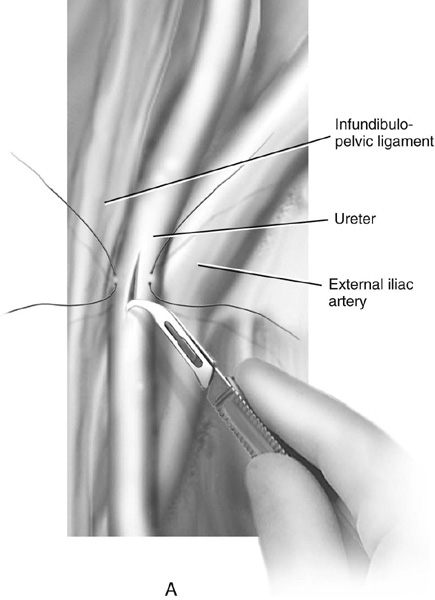
Ureterotomy and Catheterization
Ureteroureterostomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


