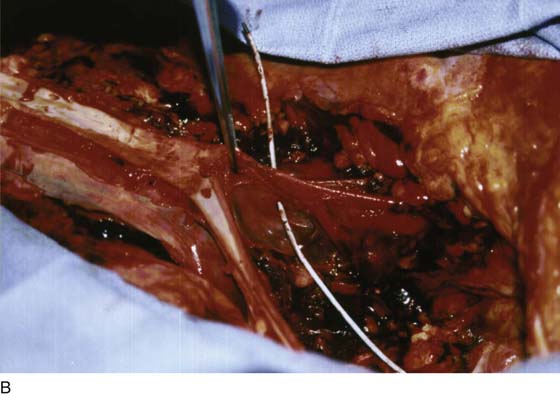
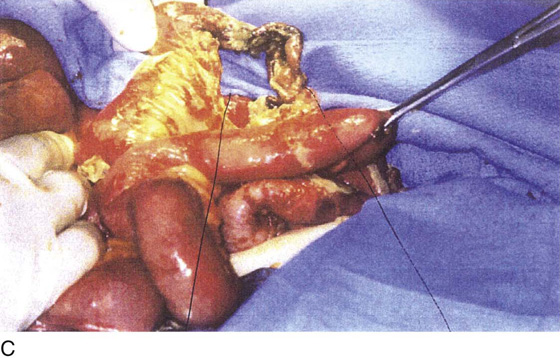
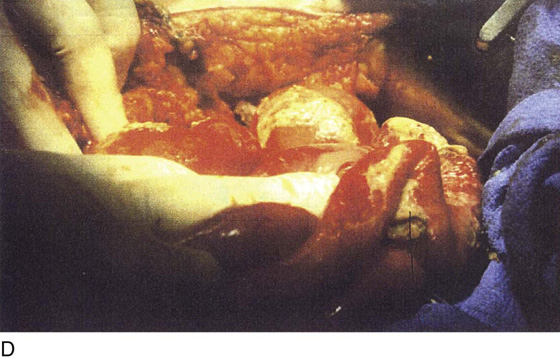
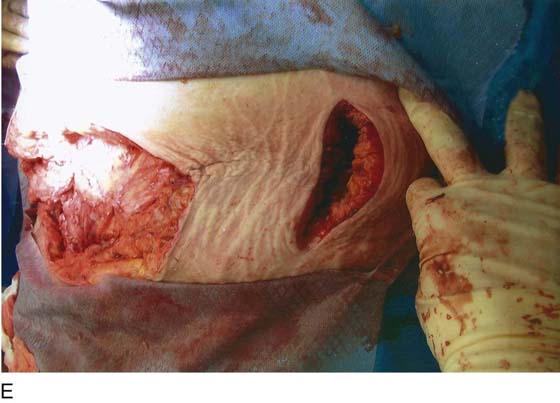
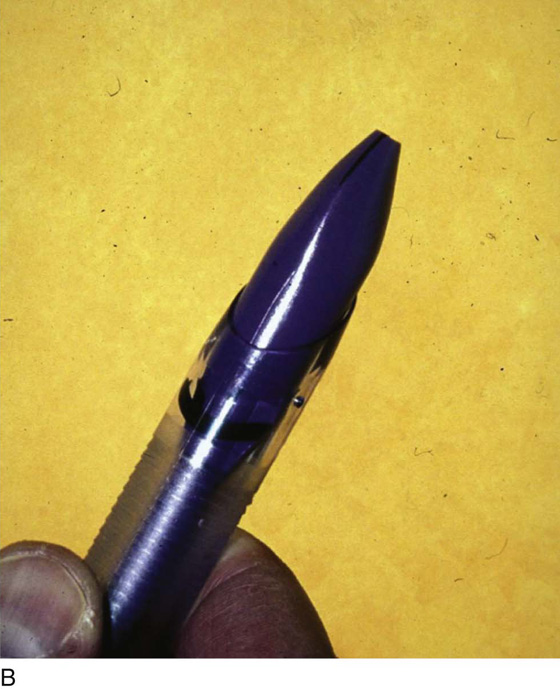
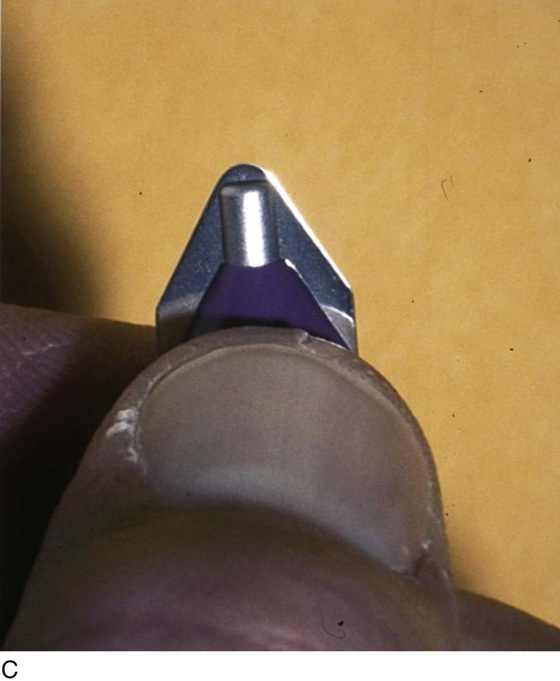
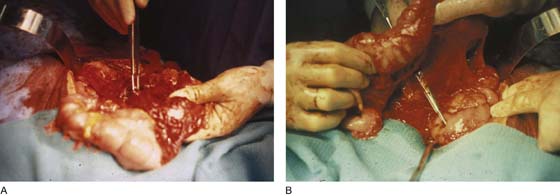
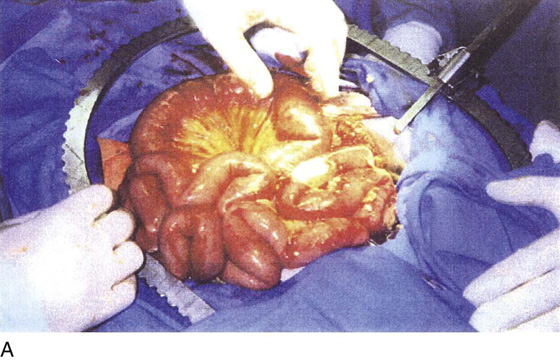
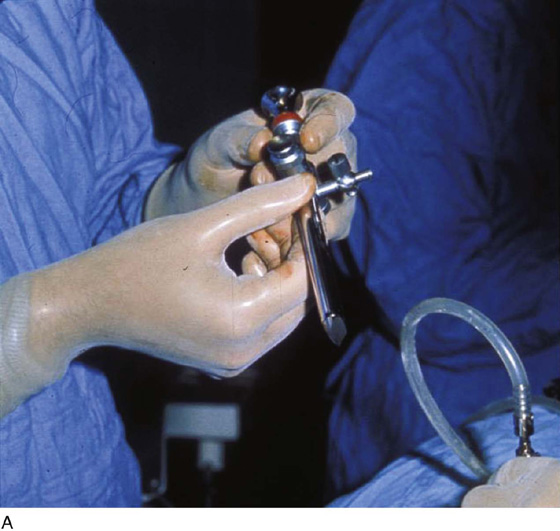
CHAPTER 122 A number of complications may be associated with laparoscopic surgery. Several of these iatrogenic injuries are unique and peculiar to the laparoscopic procedure itself (i.e., separate from the major surgical objective). For example, total abdominal hysterectomy is associated with the risk of a number of complications inherent to the surgical procedure, whereas laparoscopic hysterectomy has risks associated with the laparoscopic approach plus the hysterectomy portion of the operation. The two most serious laparoscopic complications are major vascular injury and intestinal damage. The former results in massive intra-abdominal hemorrhage and hypovolemic shock. This catastrophe must be managed in a timely, appropriate manner; otherwise, the patient will die (Fig. 122–1A through C). Small or large intestinal injury inevitably leads to immediate or delayed perforation (Fig. 122–2A, B). In some instances, significant damage to the bowel mesentery or directly to the blood vascular supply will result in ischemia followed by intestinal necrosis (Fig. 122–3A through D). As bowel contents spill into the abdominal cavity and then into the bloodstream, infection and sepsis follow. Sepsis syndrome is manifested by systemic inflammatory response syndrome (SIRS) (Tables 122–1 and 122–2). A cascade of events triggered by bacteremia and bacterial endotoxins and exotoxins eventuates in multiorgan failure. Necrotizing fasciitis may further complicate the picture in these cases. The condition progresses rapidly and is hallmarked by inordinate wound pain with cellulitis-like signs. Radiologic studies may show air within the abdominal wall (Fig. 122–3E, F). The bottom run of the downward spiral of events is septic shock (hypotension) and death. It is most convenient to subdivide these complications into those associated with the laparoscopic approach and those associated with the operative procedure (Table 122–3). To gain access to the abdominal cavity, the laparoscope must be inserted through an appropriate sleeve or cannula (Fig. 122–4A through C). These generally range in size from 5 to 12 mm inner diameter. The sleeve is typically introduced directly by incision (usually infraumbilical) followed by dissection through the layers of tissue constituting the anterior abdominal wall. When the peritoneum is reached, it is tented up and incised or bluntly traversed. The sleeve is then introduced over a blunt trocar. This technique is described as open laparoscopy. An alternative technique introduces an inert gas (e.g., carbon dioxide) via a needle, which is thrust into the abdominal cavity. When sufficient gas has been introduced to create an adequate pneumoperitoneum, hallmarked by tympany on abdominal percussion, the sleeve is introduced into the peritoneal cavity over a sharp trocar. This is a de facto blind technique. Various alternations of the aforesaid technique have been described over the years, including a device that supposedly enables the operator to view each layer of the abdominal wall as the trocar is advanced (Fig. 122–5A, B). The basis for a “safe” trocar thrust as described in an earlier chapter in this section depends on two rules. First, the trocar must be thrust into them midline without deviation to the right or to the left of the midline (Fig. 122–6A, B). Second, the angle of entry of the trocar must be made at 45° to 60° (i.e., in the direction of the uterus) (Fig. 122–7). Deviation from these key provisions will ultimately lead to disastrous consequences for the patient and her physician. Individuals at the extremes of body mass index (i.e., the very lean and the obese) are particularly at risk for iatrogenic injury (Tables 122–4 and 122–5). The obese patient is the most high-risk patient, particularly if she has had prior intra-abdominal surgery and is likely to have adhesions (Tables 122–6). Trocar entry for these women may be difficult (Fig. 122–8 and 122–9). The surgeon should not resort to the use of extra long trocar devices (11 inches in length) (Fig. 122–10); these instruments are not necessary because a trocar of standardized length (8 inches in length) is more than adequate to gain entry (Fig. 122–11). The surgeon is better advised to perform a laparotomy if a trocar of standard length is unable to provide entry into the abdominal cavity. A trocar that is thrust to the right or left of the midline may injure the iliac vessels or the vena cava (Fig. 122–12). A trocar that is thrust downward at 90° can and will injure the aorta or the left common iliac vein. Any primary trocar thrust has the potential for perforating the small intestines, whereas a deviant thrust may penetrate the large bowel (Fig. 122–13A). Because secondary trocars are placed under direct vision, injuries caused by these devices should not occur (Fig. 122–13B). FIGURE 122–1 A. Autopsy of a young women who sustained a through and through trocar injury of the left common iliac artery and died of massive blood loss. The area below the forceps shows the laceration on the posterior wall of the artery. B. The probe passed by the coroner enters the posterior wall of the artery and exits through the anterior wall. Vascular clips can be seen on the left common iliac vein. C. The probe points to a laceration in the left common iliac vein. This was the fatal wound. FIGURE 122–2 A. The forceps has been placed in a trocar wound of the omentum. B. The transverse colon has been elevated, permitting the scissors to trace the trajectory into a trocar-induced perforation of the duodenum. FIGURE 122–3 A. This 28-year-old para 3-0-0-3 underwent a postlaparoscopy emergency laparotomy. At the time of the laparotomy, the patient had extensive peritonitis and multiple small-bowel interloop abscess formations. Note the swollen, edematous small intestine. The patient also exhibited clinical signs of septic shock. B. The mesentery of the small intestine had been coagulated by plasma kinetic forceps and torn away from the intestine by blunt dissection during attempted adhesiolysis. Note the extensive ischemic and necrotic small bowel. C. Close-up at the necrotic segment of the small intestine shown in Fig. 122–3B. D. The small bowel is covered with fibrin secondary to extensive peritonitis. E. Necrotizing fasciitis is a byproduct of intestinal perforation and sepsis, particularly in obese patients. Group “A” streptococci or methicillin-resistant staphylococci rapidly spread along tissue planes while their toxins digest fat and fascia. This is clearly shown in this photo. The fat becomes grayish as the tissue undergoes cell death. F. Treatment consists of radical debridement of all dead or dying tissue. Frequent returns to the operating room are the rule before the infection is terminated. In this photo most of the fat of the anterior abdominal wall is gone, including the rectus sheath. FIGURE 122–4 A.
Major Complications Associated With Laparoscopic Surgery
Vascular and Intestinal Injury
Laparoscopic Approach



![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


