Fig. 8.1
(ESHRE/ESGE U5b/C4/V4) Complete aplasia of the uterus and upper two-thirds of the vagina. (a) Sagittal (b) axial T2WI images show complete aplasia of the uterine corpus, cervix and upper two thirds of the vagina, with fatty tissue present in the expected location of these structures (arrows in a and b). The complete failure of Mullerian development characterizes the Mayer-Rokitansky Kuster-Hause syndrome. Note presence of an ectopic pelvic kidney. Associated renal anomalies are common and MRI can provide a quick overview of the retroperitoneum and renal fossa in a single examination. The normal ovaries are visualized in a coronal T2W image (arrow in c)
Fig. 8.2
(ESHRE/ESGE U5a/C4/V4) Partial aplasia of the uterus and vagina. (a) Sagittal T2 weighted image shows aplasia of the lower uterine segment and cervix and upper third of the vagina, with an isolated uterine body and fundus with functional endometrial cavity. Note vaginal gel in the lower two thirds of the vagina (white arrow). On sagittal images, the urethra is the anatomic landmark used utilized to separate the upper (above the urethra) from the lower vagina. (b, c) Sagittal T1 weighted images with fat suppression show hematometra (black arrow in b), hematosalphynx (white arrow in c) and endometrioma (black arrow in c)
Fig. 8.3
(ESHRE/ESGE sub-class V4) Aplasia of the upper two thirds of the vagina. (a) Sagittal T2WI and (b) Sagittal T1WI with fat suppression show large hematometra, with significant distention of the endometrial cavity and cervical canal with hemorrhagic material (arrows). (c) Axial T1W1 shows absence of the vagina between the urethra and rectum
Fig. 8.4
(ESHRE/ESGE U5) Uterine hypoplasia. (a) Sagittal and (b) axial T2WI images show a small rudimentary uterus and cervix, with preservation of the zonal anatomy. The endocervical and endometrial canal are depicted as thin T2-hyperintense (arrows) line within the rudimentary uterus
Hemi-uterus (ESHRE/ESGE U4)
This type of anomaly occurs in about 10 % of cases [3, 13], and encompasses all types of unilaterally formed uterus (formly “unicornuate” uterus) [10]. There is an asymmetric failure of development of one of the Müllerian ducts, with the formation of an elongated uterus uterine horn, generally shifted to one side of the pelvis, which communicates with a normal vaginal canal. MR imaging typically shows a “banana”-shaped uterus in one side of the pelvis, with or without an associated rudimentary horn (Fig. 8.5) [7, 13]. In about 65 % of cases, there is an associated rudimentary horn which may contain functional endometrial tissue or not. The cavity of the rudimentary horn can communicate with the contralateral endometrial cavity in about 10 % of cases [3]. The diagnosis is usually made incidentally during the investigation of infertility. If a rudimentary functioning, non-communicating horn is present, there is retrograde menstrual flow and the diagnosis usually occurs at menarche with the clinical picture of dysmenorrhea and hematometrium [13, 14]. If functional endometrium is present within a non-communicating rudimentary horn, MR will show a distented uterine remnant filled with hemorrhagic material consistent with hematometra (Fig. 8.6). These patients have a greater risk of developing endometriosis, ectopic pregnancies, and obstetric complications [13, 14]. In about 40 % of the cases, associated renal anomalies occur, the most common of which is renal agenesis [14], ipsilateral to the rudimentary horn [11].
Fig. 8.5
(ESHRE/ESGE U4b) Hemi-uterus with a non-functional rudimentary horn. (a) Sagittal and (b) axial T2WI images show a hemi-uterus displaying normal zonal anatomy. A small rudimentary non-cavitary horn is present on right (arrow)
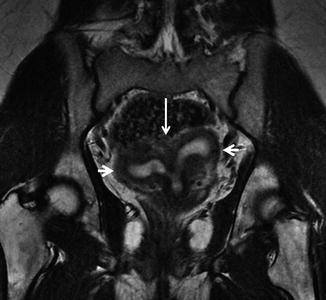
Fig. 8.6
(ESHRE/ESGE U4a) Hemi-uterus with an obstructed cavitary rudimentary horn. (a) Coronal T2WI and (b) axial T2WI show a “banana”-shaped uterus to the left of midline consistent with a hemi-uterus (formerly “unicornuate” uterus). A cavitary rudimentary horn is seen on right (long arrows), which is non-communicating resulting in hematometra. Normal ovaries are present (short arrows)
Complete Bicorporeal Uterus (ESHRE/ESGE U3b)
In this anomaly there is complete failure of fusion of the Mullerian ducts, with formation of two separate uteri with distinct endometrial cavities and cervices, which characterizes the complete bicorporeal uterus (ESHRE/ESGE U3b/C2), the formerly “Didelphys uterus” [10]. In 75 % of cases, there is a complete or partial longitudinal vaginal septum associated. The presence of vaginal septum may lead to the development of hematometrocolpos, increasing the risk of endometriosis [13, 14]. In patients with transverse vaginal septum and obstruction of one hemi-vagina, the association with ipsilateral renal agenesis is very common [13, 15]. When there is no vaginal obstruction, the patient is usually asymptomatic. If there is obstruction, the diagnosis is often made at menarche, with cyclic pelvic pain and enlarging abdominal girth. On speculum examination, a blocked hemivagina can be identified. MRI shows two separate uteri with normal endometrial-myometrial interface and preserved zonal anatomy (Fig. 8.7). The diagnosis of longitudinal vaginal septa is easily made with the use of vaginal gel or when there is an obstructed hemivagina distended by hematocolpos (Figs. 8.8 and 8.9).
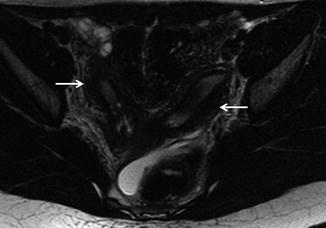
Fig. 8.7
(ESHRE/ESGE U3b/C2) Complete Bicorporeal uterus (Formerly “didelphys” uterus). Axial T2WI shows two completely separate uteri and cervices in each side of the pelvis (arrows), displaying normal zonal anatomy
Fig. 8.8
(ESHRE/ESGE U3b/C2/V2) Complete Bicorporeal uterus (formerly “dildephys”) with obstructing longitudinal vaginal septum. (a) Sagittal T2WI to the left of midline shows large hematocolpus (HC) and hematometra on the left (LU left uterus). (b) Sagittal T2WI to the right of midline shows a separate right uterus (RU) with normal zonal anatomy. The right hemivagina is distended with vaginal gel and is hyperintese (white) on T2Weighted images (arrow). (c) Coronal T2WI shows the obstructed left-hemivagina (LV) with hematocolpus (HC) and hematometra (LU left uterus). The normal right hemi-vagina distended with gel (arrow). (d) Direct examination shows normal right hemivagina (RV) and right cervical os (arrow). The obstructed left hemivagina (LV) is seen on the left (HC)
Fig. 8.9
(ESHRE/ESGE U3b/C2/V2) Bicorporeal uterus (didelphys) with obstructed right hemi-vagina. (a) Coronal T2WI two divergent completely separate uteri and cervices, consistent with complete bicorporeal uterus (didelpys) (RU right uterus and LU left uterus). There is an obstructing longitudinal vaginal septum, and the right hemi-vagina is obstructed and disdented with hemorrhagic material (RV right vagina). (b) Sagittal T1WI with fat suppression shows the extensive right hematocolpus (RV right vagina). (c, d) Axial T2WI images following surgery show two normal separate uteri (arrows in c) and two separate hemi-vaginas distended with gel, separated by a longitudinal septum (arrow in d)
Bicorporeal Uterus (ESHRE/ESGE U3)
In this anomaly, there is incomplete fusion of the Mullerian ducts, forming two symmetrical horns, which merge caudally usually in the isthmus, forming a bicorporeal uterus with normal cervix (ESHRE/ESGE U3), the formerly “Bicornuate” uterus. The bicorporeal uterus may be partial (class U3a) or complete (class U3b), depending on the degree of separation of the uterine corpus by the external fundal indentation [10]. It occurs in approximately 10 % of cases [12, 13]. Both uterine horns are divergent (intercornual distance greater than 4.0 cm) and there is a deep cleft between the horns (exceeding 50 % of the uterine wall thickness) (10). Patients are usually asymptomatic; however, there is a high rate of associated obstetric complications [3, 12]. MR demonstrates noninvasively the outer contour of the uterine fundus, with two divergent uterine horns, and a large fundal indentation (exceeding 50 % of the uterine wall thickness) between them (Fig. 8.10). The zonal anatomy is preserved in both horns. Associated pathologies such as leiomyoma and adenomyosis are also easily identified. In a bicornuate-bicoli uterus there is some communication between the horns, unlike didelphic uterus where the uteri are completely separate.