Macrosomia
Roya Sohaey, MD
DIFFERENTIAL DIAGNOSIS
Common
Idiopathic Macrosomia
Diabetes
Less Common
Hydrops
Rare but Important
Beckwith-Wiedemann Syndrome
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Large for gestational age fetus
↑ Estimated fetal weight (EFW)
> 90th or 95th percentile
Birth weight > 4,000-4,500 g
AC alone can predict macrosomia
37% risk of macrosomia if AC > 37 cm
< 1% risk of macrosomia if AC < 35 cm
AC often 1st measurement to ↑
↑ Glycogen stores in liver
Truncal obesity
Prevalence
16-18% in diabetics
6-8% in non-diabetics
Helpful Clues for Common Diagnoses
Idiopathic Macrosomia
No fetal anomalies
Hereditary factors (↑ risk if mom is large)
1/3 with polyhydramnios
Diabetes
Polyhydramnios common
Associated anomalies
Caudal dysplasia/regression
Open neural tube defect
Cardiac anomalies (5x ↑ risk)
Polydactyly
GU/GI anomalies
Single umbilical artery
Helpful Clues for Less Common Diagnoses
Hydrops
Immune and nonimmune causes
Excessive body fluid large fetus
large fetus
Anasarca ± cystic hygroma
Pleural effusion
Ascites
Helpful Clues for Rare Diagnoses
Beckwith-Wiedemann Syndrome
Signs/symptoms
Macroglossia
Enlarged internal organs (especially kidneys)
Hemihypertrophy
Omphalocele
Prognosis
20% infant mortality
7-10% tumor risk (Wilms tumor most common)
Other Essential Information
Fetal complications of macrosomia
Shoulder dystocia (10%)
Asphyxia
Hypoglycemia, hypocalcemia
Macrosomia associated with polyhydramnios
Image Gallery
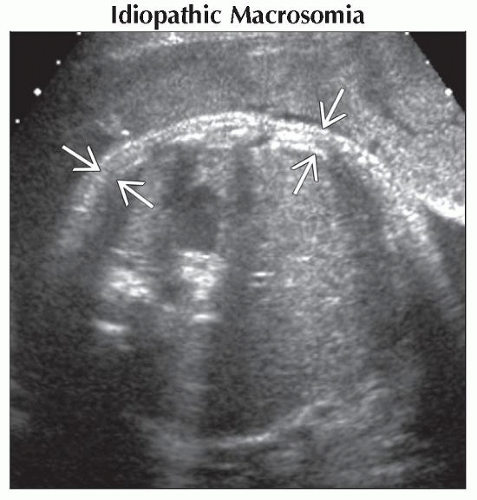 Axial ultrasound of the fetal abdomen shows increased truncal subcutaneous fat
 . The abdominal circumference measurement was 5 wks greater than the other fetal biometric measurements. . The abdominal circumference measurement was 5 wks greater than the other fetal biometric measurements.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|