Fig. 7.1
Theater layout, personnel, and stack position for a right pyeloplasty

Fig. 7.2
Patient position in laparoscopic approach for left pyeloplasty
4.
First port is placed by an open technique (Hasson) in the region of the umbilicus and secured with a skin suture. The gas flow is set at 2–4 L/min and the abdominal pressure at 10–12 mmHg. Two working ports are inserted under direct vision: one under the costal margin and the other in the ipsilateral iliac fossa (Fig. 7.3 ). The position of this latter port (# 3), which is used for the needle holder, is crucial, as it has to be in line with the anastomosis to facilitate suturing.

Fig. 7.3
Port positions: one in the umbilicus, one under the costal margin, and a third in the ipsilateral iliac fossa
5.
The kidney is identified by reflecting the colon medially or through a trans-mesenteric window in the left side in suitable cases (Fig. 7.4).
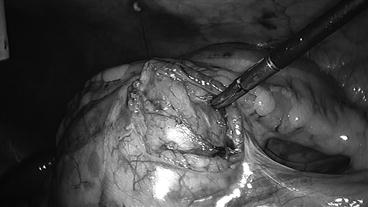
Fig. 7.4
PUJ access through a trans-mesenteric window in the left side
6.
Gerota’s fascia is incised, and the PUJ is identified.
7.
The renal pelvis is stabilized with a “hitch stitch” by passing a straight needle (3/0 or 4/0 Prolene) or a regular 5/0 Prolene in small infants passing directly through the abdominal wall and/or through a fourth 3 mm trocar (Fig. 7.5 ).
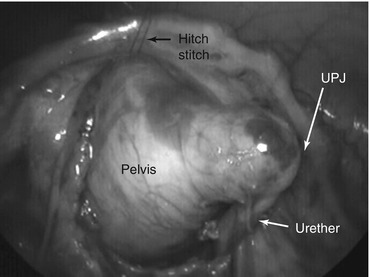
Fig. 7.5
A “hitch stitch” is use to stabilize the renal pelvis
8.
The renal pelvis is dismembered and a portion of the redundant dilated part could be excised. The ureter is spatulated, and if necessary, it can be stabilized with another “hitch stitch,” similar than the pelvis.
9.
The anastomosis is performed with 6/0 Monocryl® on a round body needle. The inferior part of the anastomosis is sutured first with an 8–10 cm length of suture. The remainder of anastomosis is performed with a running suture 10–12 cm long.
10.
After suturing the posterior wall and starting the anterior wall, a transanastomotic stent is placed either through the fourth trocar or directly through the abdominal Wall using a 19 GA Teflon cannula. A guidewire is passed down the ureter and into the bladder. Then a double-J stent is advanced over the guidewire with vaseline oil and placed between the renal pelvis and the bladder. When this maneuver is done through a cannula, there is no possibility of using an extra instrument, which is very useful especially during learning curve.
11.
The remainder of the anastomosis is completed with a further continuous suture of 6/0 Monocryl® of the same length.
12.




The “hitch stitch” is removed, and the anastomosis is placed in normal anatomical position. The colon is replaced without a suture, and the mesenteric window is closed if a trans-mesenteric approach was used.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
