Chapter 504 Isolated Glomerular Diseases with Recurrent Gross Hematuria
504.1 Immunoglobulin A Nephropathy (Berger Nephropathy)
Pathology and Pathologic Diagnosis
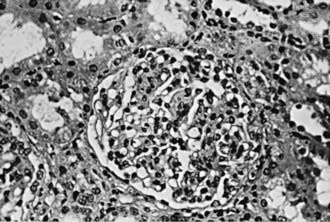
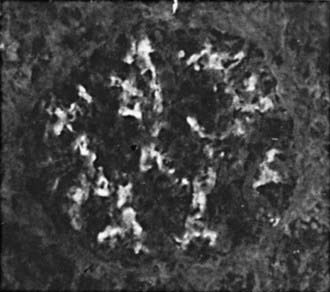
Focal and segmental mesangial proliferation and increased mesangial matrix are seen in the glomerulus (Fig. 504-1). Renal histology demonstrates mesangial proliferation that may be associated with epithelial cell crescent formation and sclerosis. IgA deposits in the mesangium are often accompanied by C3 complement (Fig. 504-2).