International Pediatric Ophthalmology
Sherwin J. Isenberg and Leonard Apt
EPIDEMIOLOGY
Approximately 500,000 children become blind worldwide each year. This figure represents one new case of pediatric blindness every minute. It has been estimated that today there are 1,400,000 blind children in the world,1 and many of these children will not survive beyond 2 years of age. While 1,000,000 are considered untreatable by current standards due to retinal dystrophy, microphthalmos, cortical blindness, and optic atrophy or hypoplasia, the remaining 400,000 cases are potentially treatable. The main avoidable causes are corneal scarring from infection or trauma (260,000), cataract (50,000), and retinopathy of prematurity (ROP; 40,000).2 Other treatable blinding conditions include amblyopia and uncorrected refractive error. Much of the data concerning causes of pediatric blindness in developing countries come from studies of children attending schools for the blind. This information may represent a bias, since data from children not attending these schools would not be included.
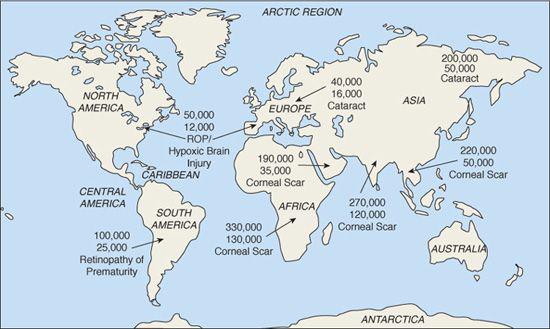
In developed areas, the main causes of pediatric blindness are ROP, perinatal hypoxic brain injury, optic nerve hypoplasia, inherited retinal dystrophies, congenital anomalies, cataract, and glaucoma. These disorders are largely not preventable, but some are treatable. Geographically, 90% of all pediatric blindness (1,300,000) occurs in developing countries with 24% in Africa, 20% in India, and 29% in the rest of Asia (Fig. 582-1). In these areas, the major causes of childhood blindness are vitamin A deficiency, trachoma, ophthalmia neonatorum, measles infection, harmful traditional medicines, and trauma. All these conditions are largely the result, directly or indirectly, of malnutrition, lack of sanitation, or infection, and most of these factors cause blindness primarily through corneal scarring. All of these conditions are preventable or treatable. Blindness in children due to uncorrected major refractive errors occurs in 0.6% to 2.6% of children in developing areas. In China, it is thought that nearly 6 millions children are visually impaired simply because they are in need of glasses that they may never receive.3
In some areas of the world, there are more specific localized causes of blindness. For example, in Brazil, endemic toxoplasmosis is very common and often results in bilateral macular scars with resultant legal blindness. In Uganda, rubella-related congenital cataract is frequently encountered. In Sri Lanka and many areas of the Middle East, genetic diseases resulting from consanguinity can often be found, explaining the relatively high prevalence of infantile glaucoma, retinal degenerations, and infantile cataract. In other locations, especially nontropical, semideveloped areas, the major etiologies of childhood blindness are similar to developed regions.
A contributing factor to worldwide childhood blindness is an inadequate number of pediatric ophthalmologists. General ophthalmologists may not want to operate on infants. In addition, anesthesiologists in these areas are often reluctant to anesthetize small infants. Thus, many children go untreated for ROP, cataracts, glaucoma, and treatable blinding disorders. For pediatric ophthalmologists, early infancy is often the most favorable period to surgically improve glaucoma, cataract, and structural defects. For example, in the People’s Republic of China, there are about 200,000 blind children (Fig. 582-2).4 Of them, 22.5% (45,000) have cataract, glaucoma, ROP, and uveitis and are thus potentially treatable. At least in China, the situation is improving with more advanced physician training and alteration of hospital policies regarding surgery on infants.
PREVENTION AND INTERVENTION
It may appear relatively easy to conceive strategies to combat blindness, since the causes are often single, identifiable, and uncomplicated. In regions with a high prevalence of rubella, vaccination would be beneficial. Yet, the price for a nationwide vaccination program is often too expensive to consider. Toxoplasmosis prevention is difficult in areas with a dense population and many pets. Discouraging consanguinity may be complicated by social and religious mores. In areas with inadequate numbers of professionals in the field, the proper training of pediatric ophthalmologists, nurses, and other health workers will reduce treatable blindness in the future, but there are financial, geographic, and access issues that make training new workers a challenge. The widespread distribution of vitamin A, especially where there is malnourishment, will greatly help to prevent corneal blindness, both primary blindness due to the deficiency and secondary blindness due to infection, as would better nutrition.
In developing countries, the most common treatable cause of pediatric blindness is infection. Antibiotics are often not an option due to lack of availability and relatively high cost. For use in developing countries, an antimicrobial agent would need to meet certain criteria, including effectiveness against bacteria and other microbes, safety, widespread availability, and ease of preparation. Importantly, it must not be expensive. Povidone-iodine meets these criteria. It is effective against all bacteria, viruses, and fungi in vitro (given enough contact time) and causes few allergic reactions. It is questionable whether true bacterial resistance to povidone-iodine even exists.5 It can be prepared from preexisting powders or solutions, which are available worldwide and are very cheap. In Kenya, a 5 mL bottle of the solution costs less than $0.10 to prepare.6 In addition, the povidone-iodine solution colors the eye brown for about 2 minutes, confirming proper administration.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


