Chapter 338 Inguinal Hernias
Embryology and Pathogenesis
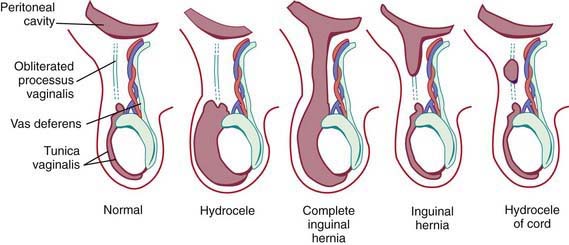
Androgenic hormones, adequate end-organ receptors, and mechanical factors such as increased intra-abdominal pressure influence complete descent of the testis through the inguinal canal. The testes and spermatic cord structures (spermatic vessels and vas deferens) are located in the retroperitoneum but are affected by increases in intra-abdominal pressure as a consequence of their intimate attachment to the processus vaginalis. The genitofemoral nerve also has an important role: It innervates the cremaster muscle, which develops within the gubernaculum, and experimental division or injury to both nerves in the fetus prevents testicular descent. Failure of regression of smooth muscle (present to provide the force for testicular descent) might have a role in the development of indirect inguinal hernias. Several studies have investigated genes involved in the control of testicular descent for their role in closure of the patent processus vaginalis, for example, hepatocyte growth factor and calcitonin gene-related peptide. Unlike in adult hernias, there does not appear to be any change in collagen synthesis associated with inguinal hernias in children (Fig. 338-1).
Pathology
A hydrocele is when only fluid enters the patent processus vaginalis and the swelling may exist only in the scrotum (scrotal hydrocele), only along the spermatic cord in the inguinal region (hydrocele of the spermatic cord), or extend from the scrotum through the inguinal canal and even into the abdomen (abdominal-scrotal hydrocele). A hydrocele is termed a communicating hydrocele if it demonstrates fluctuation in size, often increasing in size after activity and, at other times, being smaller when the fluid decompresses into the peritoneal cavity. Occasionally, hydroceles in older children follow trauma, inflammation, or tumors affecting the testis. Although reasons for failure of closure of the processus vaginalis are unknown, it is more common in cases of testicular nondescent and prematurity. In addition, persistent patency of the processus vaginalis is twice as common on the right side, presumably related to later descent of the right testis and interference from the developing inferior vena cava and external iliac vein. Risk factors identified as contributing to the development of congenital inguinal hernia relate to conditions that predispose to failure of obliteration of the processus vaginalis and are listed in Table 338-1. Incidence of inguinal hernia in patients with cystic fibrosis is ~15%, believed to be related to an altered embryogenesis of the wolffian duct structures, which leads to an absent vas deferens in males with this condition. There is also an increased incidence of inguinal hernia in patients with testicular feminization syndrome and other forms of ambiguous genitalia. The rate of recurrence after repair of an inguinal hernia in patients with a connective tissue disorder approaches 50%, and often the diagnosis of connective tissue disorders in children results from investigation after development of a recurrent inguinal hernia.



