Chapter 319 Ingestions
319.1 Foreign Bodies in the Esophagus
Evaluation of the child with a history of foreign body ingestion starts with plain anteroposterior (AP) radiographs of the neck, chest, and abdomen, along with lateral views of the neck and chest. The flat surface of a coin in the esophagus is seen on the AP view and the edge on the lateral view (Fig. 319-1). The reverse is true for coins lodged in the trachea; here, the edge is seen anteroposteriorly and the flat side is seen laterally. Disk batteries can look like coins (Fig. 319-2) and have a much higher risk of burns and necrosis (Fig. 319-3). Materials such as plastic, wood, glass, aluminum, and bones may be radiolucent; failure to visualize the object with plain films in a symptomatic patient warrants urgent endoscopy. Although barium contrast studies may be helpful in the occasional asymptomatic patient with negative plain films, their use is to be discouraged because of the potential of aspiration as well as making subsequent visualization and object removal more difficult.


Figure 319-2 Disk battery impacted in esophagus. Note the double rim.
(From Wyllie R, Hyams JS, editors: Pediatric gastrointestinal and liver disease, ed 3, Philadelphia, 2006, Saunders.)
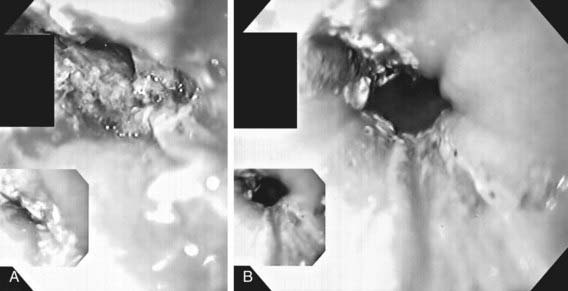
Treatment of esophageal foreign bodies usually merits endoscopic visualization of the object and underlying mucosa and removal of the object; therapeutic endoscopy is most conservatively done with an endotracheal tube protecting the airway. Sharp objects in the esophagus, disk button batteries, or foreign bodies associated with respiratory symptoms mandate urgent removal. Button batteries, in particular, must be expediently removed because they can induce mucosal injury in as little as 1 hr of contact time and involve all esophageal layers within 4 hr (see Fig. 319-3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


