Fig. 1
Normal appearance of the proximal humeral physis in a 6-year-old boy. (a) On the AP internal rotation view, the physis has an oblique orientation, which can be easily mistaken for a fracture. (b) On the AP external rotation view, however, it is clear that the physis (arrow) and humeral contours are intact, without discontinuity that would suggest fracture
Table 1
C-R-I-T-O-E, the mneumonic for the order of ossification of the apophyses about the elbow joint, is as above (Iyer 2012)
Ossification center | Age (years) of appearance on radiograph, girls | Age (years) of appearance on radiograph, boys |
|---|---|---|
C – Capitellum | 1 | 2 |
R – Radial head | 3 | 4 |
I – Inner (medial) epicondyle | 5 | 6 |
T – Trochlea | 7 | 8 |
O – Olecranon | 9 | 10 |
E – External (lateral) epicondyle | 11 | 12 |
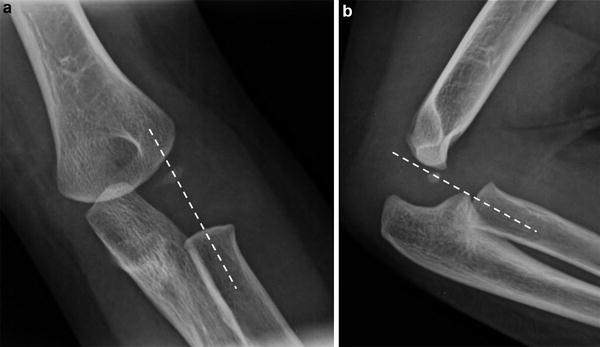
Fig. 2
Normal radiocapitellar relationship. Line drawn through neck of the radius should bisect the capitellum on frontal (a) and lateral (b) radiographs
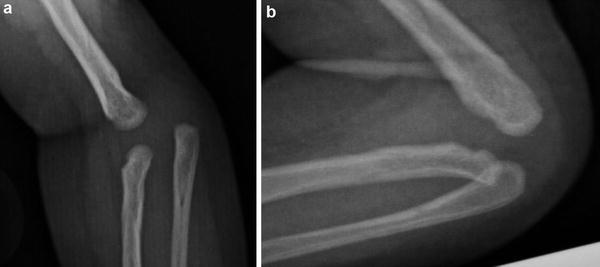
Fig. 3
Congenital radial head dislocation. Frontal (a) and lateral (b) radiographs of the elbow demonstrate disruption of the radiocapitellar line. Additionally, the radial head is deformed with a convex superior border, suggesting congenital etiologies
Congenital dysplasias are best demonstrated by plain radiography (Lachman 2008) (Fig. 4).

Fig. 4
Select congenital abnormalities of the upper extremity in children. (a) Carpal coalition involving the lunate and triquetrum (arrow). (b) Polydactyly, with an accessory digit that extends from the thumb and contains rudimentary phalanges. (c) Apert’s syndrome, with soft tissue and osseous syndactyly (“mitten-hand”) deformity that is typical of this syndrome. (d) Radial ray anomaly, with absent radius and foreshortening of the humerus. (e) Chondrodysplasia punctata. Note stippled calcification of the articular cartilage of the upper extremities with rhizomelic pattern of limb shortening
Plain radiographs are also the mainstay of imaging to evaluate trauma. Cross-sectional modalities are only utilized in select instances (Fig. 5).

Fig. 5
Elbow fractures in children. (a) Supracondylar fracture (arrow) results in a large joint effusion as well as anterior displacement of the distal humeral fracture fragment, which includes the capitellum. (b) A medial epicondylar avulsion fracture (arrow) occurs in the 7–15-year age group and, due to disruption of the cartilage between the epicondyle and the condyle, is either a Salter-Harris 3 or 4 fracture (Iyer 2012). (c) Lateral condylar fracture (arrow) is seen as sliver of fractured bone along the lateral condyle of distal humerus. There is no disruption of the anterior humeral line as seen on lateral view, unlike a supracondylar fracture
Periosteal reaction is most commonly seen in the setting of healing fracture; however, it also present in a wide variety of benign and malignant conditions (Rana et al. 2009) (Table 2 and Fig. 6).

Table 2
Periosteal reaction is the bone’s response to many different causative etiologies. The appearance on radiograph can be characteristic of either a benign or a malignant process
Type of periosteal reaction | Radiographic example | Etiologies | |
Benign | Smooth |  | Physiologic |
Symmetric | Prostaglandin-induced | ||
Solid | |||
Thermal injury | |||
Healing fracture | |||
Sickle Cell Disease | |||
Scurvy | |||
Leukemia | |||
Caffey’s Disease | |||
Malignant | Spiculated |  | Osteogenic sarcoma |
Langerhan’s Cell Histiocytosis (LCH) | |||
Infection | |||
Lamellated | Ewing’s Sarcoma | ||
LCH | |||
Infection | |||
Codman’s Triangle | Osteogenic sarcoma | ||
LCH | |||
Infection | |||
Amorphous/disorganized | 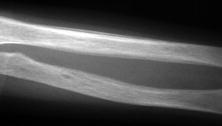 | LCH | |
Infection | |||
Fig. 6
Periosteal reaction. (a) Prostaglandin therapy can result in solid periosteal reaction in the neonate. (b) In this 2-year-old who suffered a severe thermal injury, smooth periosteal reaction is identified along the humeri. (c) Dactylitis is a common finding in sickle-cell patients, the result of “extensive infarction of the marrow, medullary trabeculae and the inner layers of the cortical bone [with] subsequent circumferential periosteal elevation and formation of subperiosteal new bone” (Babhulkar 1995, p. 312). (d) In this patient with large cell lymphoma, amorphous periosteal reaction is identified with an underlying moth-eaten appearance to the bony matrix, indicating a malignant process
While cross-sectional imaging and radionuclide imaging are the most sensitive and specific in the evaluation of infection of the bones and soft tissues of the extremities, plain radiography remains the first-line imaging modality as the presence of findings will prevent delays in treatment. For some infectious organisms, most notably in congenital syphilis, characteristic radiographic findings such as destructive metaphyseal lytic lesions may aid in the diagnosis (Shore 2008) (Fig. 7). Plain radiography has a limited role in early osteomyelitis (Fig. 8); however, it is useful in the evaluation of the complications of osteomyelitis, such as premature physeal closure, joint destruction, and growth disturbance.
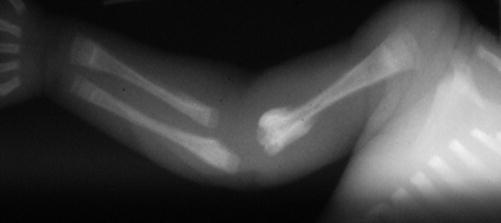
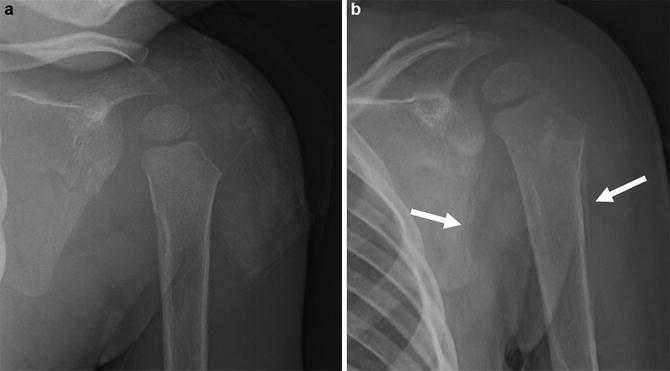
Fig. 7
Characteristic findings of congenital syphilis, including diaphysitis as well as productive metaphysitis (distal humerus) and destructive metaphysitis (proximal humerus). The alternating bands of increased and decreased density in the proximal and distal radial and ulnar metaphyses are the typical “sandwich” configurations of superimposed productive and destructive metaphysitis (Rasool and Govender 1989, p. 753)
Fig. 8
Limited role of plain films for osteomyelitis in the acute setting. (a) Patient presenting with fever, elevated white count, and refusal to move left shoulder. Plain radiograph of the left shoulder demonstrates widened glenohumeral joint space concerning for effusion without any osseous abnormality. (b) Follow-up plain radiograph obtained 2 weeks later depicts periosteal reaction adjacent to the scapula and proximal humeral diaphysis (arrows), consistent with osteomyelitis in this patient with septic joint
With inflammatory arthropathies and connective tissue disorders, plain radiographs are often obtained at diagnosis in order to evaluate for erosive changes, sclerosis, joint space narrowing, and/or distribution of disease (Brant and Helms 2007). Soft tissue calcifications may be evident in some conditions, such as dermatomyositis.
In a child with suspicion for rickets, frontal radiographs of the wrists and knees are obtained (Fig. 9) (Shore 2008). These are the sites of fastest growth and will demonstrate early findings of irregularity of the zone of provisional calcification of the physis and apparent physeal widening. In premature newborns, incidental changes from rickets involving the humeral heads may be detected on routine chest radiography.

Fig. 9
Characteristic findings in rickets. In areas of rapid bone turnover, such as the metaphyses of the distal radius and ulna, fraying and cupping occurs secondary to uncalcified bony matrix. Additionally, bones can become severely osteopenic resulting in microfractures and smooth periosteal reaction, as demonstrated in this child with rickets (Berry 1952)
Plain radiographs are also important in the evaluation of benign and malignant bone tumors. The benign or aggressive nature of the lesion can be estimated by several criteria, including the morphology, the zone of transition, the internal matrix, the appearance of periosteal reaction, the presence of cortical destruction or a soft tissue mass, the location of the lesion, and the number of lesions (Brant and Helms 2007). It should be noted that in children, Langerhans cell histiocytosis and osteomyelitis are two benign conditions that may appear aggressive/malignant on plain radiography. The differential diagnosis may become quite short on the basis of radiographs alone (see Table 2 and Figs. 10 and 11).
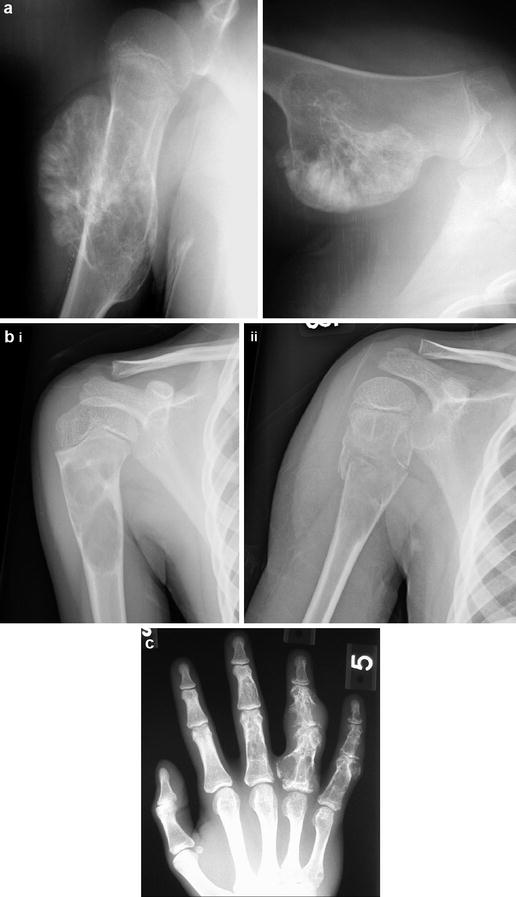

Fig. 10
Typical appearance of several benign bone tumors. (a) AP and lateral view of a sessile osteochondroma of the proximal humeral metaphysis. (b) Unicameral bone cyst without (i) and with (ii) an associated pathologic fracture and a “fallen fragment.” (c) Enchondromas of the phalanges, most prominent in the fourth digit, demonstrate the typical arcs and whirls of a chondroid matrix
Fig. 11
Large cell lymphoma. Frontal radiograph of the forearm shows permeative pattern of bone destruction in the radial and ulnar diaphysis with periostitis
In the setting of a soft tissue mass, radiographs may demonstrate secondary osseous involvement or internal calcification. Phleboliths associated with venous malformations may be apparent on plain radiographs.
Bone age evaluation is traditionally performed by plain radiography of a hand with comparison to normal standards of age and gender. The most widely used reference is the standard text by Greulich and Pyle (1959); however, there are now multiple alternatives available, most notably by Gilsanz and Ratib (2012).
MRI
Magnetic resonance imaging (MRI) is the modality of choice for musculoskeletal cross-sectional imaging in the pediatric upper extremity. Inherent advantages of MRI include excellent spatial and contrast resolution of the soft tissues and bones, which is accomplished without imparting radiation to the patient. However, the long imaging time necessary to perform a complete MRI exam can be a significant disadvantage, resulting in the need for sedation or general anesthesia in young patients who cannot lay still throughout the protracted study (Strouse 2008).
Congenital Differences
While most congenital differences of the upper extremity are assessed with plain radiographs, MRI is a useful adjunct in some instances. MRI is particularly useful in the pediatric population as the skeletal structures may still be cartilaginous and are therefore much better seen with MRI as opposed to computed tomography (CT) or plain x-ray (Strouse 2008).
An important entity diagnosed easily on MRI is glenohumeral dysplasia, which may occur in isolation or in association with mucopolysaccharidoses, mucolipidoses, or skeletal dysplasias. Injury to the brachial plexus during birth, with resulting paralysis of the shoulder girdle musculature, can also inhibit normal development of the glenoid and humeral head and thus lead to glenohumeral dysplasia (Gudinchet et al. 1995). The glenoid articular surface is deficient, particular posteriorly, and the humeral head is flattened and small. Furthermore, the humeral head is often posteriorly dislocated because of the glenoid deficiency (Fig. 12). With advances in imaging, MR neurography can be used to depict normal and abnormal peripheral nerves (Figs. 13 and 14) (Chhabra et al. 2011).
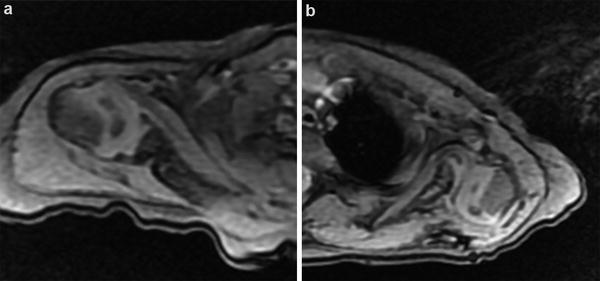
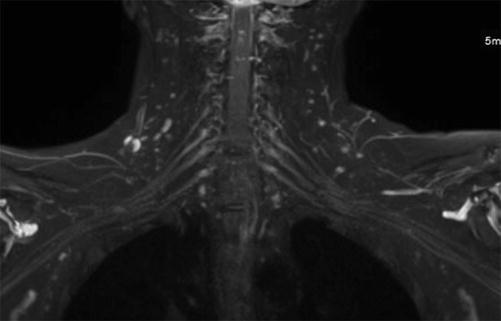
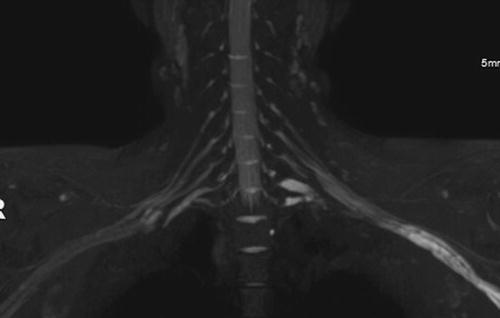
Fig. 12
Congenital glenohumeral dysplasia. MRI of bilateral shoulder joints. Axial GRE images through glenohumeral joints show (a) normal alignment in the right shoulder and (B) posteriorly subluxed humeral head with deformed, dysplastic glenoid cavity (arrow) and absent labrum in the left shoulder joint. Note globally decreased muscular caliber compared to the contralateral side
Fig. 13
Normal MR neurography appearance of the brachial plexus. Coronal MIP projection from 3D STIR SPACE image shows normal symmetrical appearance of bilateral brachial plexuses. Notice dorsal nerve root ganglions are the most hyperintense and the signal intensity and caliber of the brachial plexus segments decrease gradually along their distal course with no nerve kinking or irregularity (Courtesy: Avneesh Chhabra M.D.)
Fig. 14
MR neurography in a patient with chronic inflammatory demyelinating polyneuropathy. Young boy with multifocal motor-sensory neuropathy, worse on the left side. Coronal MIP projection from 3D STIR SPACE image shows multifocal patchy thickening and asymmetric hyperintensity of the brachial plexus, especially on the left side (Courtesy: Avneesh Chhabra M.D.)
Trauma
Osseous injury may result from a single traumatic event or due to repetitive stresses. Although conventional radiographs are the first modality utilized for evaluating osseous trauma, many acute and chronic osseous injuries are not detectable on plain radiographs. MRI is exquisitely sensitive for detection of radiographically occult injuries. A normal MRI essentially excludes the presence of an osseous injury.
Radiographically occult fracture. It is well known that MRI is able to demonstrate radiographically occult fractures in a rapid, cost-effective manner to enable optimal patient management. In such cases, in addition to demonstrating marrow edema, a fracture line is usually identified as a linear or curvilinear focus of low signal intensity on T1W images that may demonstrate low or high signal on STIR images (Fig. 15).

Fig. 15
Elbow joint dislocation with radiographically occult intra-articular fracture of ulna. Lateral (a) and frontal (b) plain radiographs demonstrate disruption of the radiocapitellar relationship with large joint effusion. Small osseous fragment (arrow) is seen in the joint space without definite donor site. The intra-articular osteochondral ulnar fracture with bone marrow edema (arrow) is seen on sagittal STIR (c) and T1 (d) images from MRI study as high and low signal, respectively. The full thickness cartilage defect is best seen on the GRE sequence (e)
MRI is also useful in the evaluation of fracture complications. For example, in the setting of a prior scaphoid fracture, MRI will show changes of avascular necrosis before plain radiographs (Fig. 16).

Fig. 16
Scaphoid fracture with avascular necrosis of the proximal pole. (a) Scaphoid fracture is seen on the plain radiograph. (b) Coronal T1 image from MRI shows scaphoid fracture (arrow) and additional finding of decreased T1 signal in the proximal pole (arrowhead) consistent with avascular necrosis
Avulsion fracture. Avulsion fractures typically demonstrate abnormal marrow signal at the site of the injury, but the extent of marrow abnormality generally is limited and appears less robust than with impaction injuries.
Repetitive trauma. Stress injuries to bone typically are divided into two categories: insufficiency and fatigue fractures (Daffner and Pavlov 1992). Fatigue fractures result from abnormal stress to normal bone and, therefore, are seen commonly in the pediatric population. Chronic avulsive injuries such as shin splints can be difficult to diagnose on plain radiographs, but can be detected with MRI.
Physeal injury . In a skeletally immature patient, trauma to the physes can result in premature closure of a portion of the physis, which results in differential growth and subsequent deformity. The diagnosis of osseous bridging can be challenging on plain radiographs. MRI with its gradient echo images, which are designed to assess the cartilage, is the gold standard for the assessment of such injuries (Carey et al. 1998).
The physes may be susceptible to chronic repetitive trauma in athletes, most characteristically the distal radius and olecranon in gymnasts and the proximal humerus in baseball pitchers. The characteristic findings on MRI include physeal widening and T2-hyperintensity at the junction of the physis and metaphysis.
Epiphyseal injury . Osteochondritis dissecans (OCD) is fragmentation or separation of a portion of subchondral bone along the articular surface. Two types of OCD have been described: the juvenile form, occurring before physeal closure, and the adult type. Common joints involved include the knee, ankle, and elbow. In the elbow, there is involvement of the capitellum along its convex anterior surface. MRI is used in the evaluation for instability, as well as osseous or cartilaginous loose bodies within the joint. Linear T2-hyperintense signal between the osseous fragment and the parent bone is suggestive of instability (Fig. 17). The capitellum is also susceptible to avascular necrosis, called Panner’s disease. This disease is most commonly seen in children with repeated valgus stress to the elbow, such as baseball players and gymnasts. The entire capitellum is affected, becoming diffusely T1-hypointense on MRI. Children with Panner’s disease are typically younger than those with an osteochondral injury.
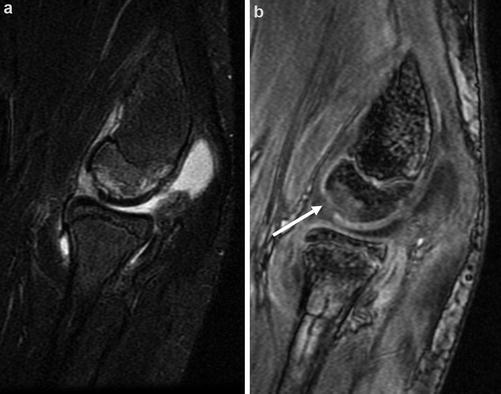
Fig. 17
Osteochondritis dissecans. MRI of the elbow with sagittal STIR (a) and sagittal GRE (b) images demonstrates osteochondral lesion involving the anterior articular surface of the capitellum with high T2 signal. The full thickness cartilage defect is better seen on the gradient sequence (arrow)
Soft tissue injuries. An added advantage of MRI is its ability to demonstrate soft tissue injuries, including injuries to the ligaments, tendons, and cartilage that may mimic a fracture clinically (El-Khoury et al. 1996). MR arthrography refers to distention of the joint with a solution containing dilute gadolinium (contrast agent). It is extremely useful in assessing intra-articular soft tissue injuries in the shoulder and hip (Waldt et al. 2005). A common labral injury seen in the setting of an anterior shoulder dislocation is the Bankart tear (Stoller 1997) (Fig. 18).
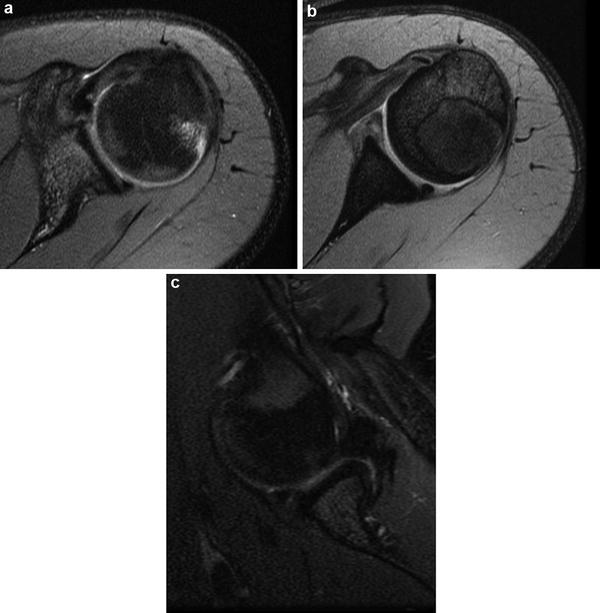
Fig. 18
Bankart lesion with Hill Sachs’ deformity. (a) Axial PD FS image at the level of the superior glenohumeral joint depicts high T2 signal with deformity of the posterolateral humeral head (arrow), consistent with Hill Sachs’ deformity. (b) Axial PD FS image at the level of the inferior glenohumeral joint depicts anterior labral tear with disruption of the periosteum (arrow). C. PD FS image obtained with the patient in ABER (abduction and external rotation) confirms the displaced anterior labral tear, consistent with Bankart lesion
Some other uses of MRI in the setting of trauma include ligament tears in the elbow and wrist. Scapholunate ligament and triangular fibrocartilage (TFCC) tears are optimally evaluated for on MRI (Fig. 19).

Fig. 19
Tear of the triangular fibrocartilage (TFCC). MRI of the wrist with coronal T1 (a) and coronal GRE (b) images demonstrates signal abnormality within the body of the triangular fibrocartilage (TFCC), consistent with a tear
Infection
Musculoskeletal infections can affect bones, soft tissues, and joints. Although MRI diagnosis of osteomyelitis does not require contrast, use of contrast does increase the confidence of the radiologist in providing the diagnosis and aids in the assessment of complications such as abscesses (Averill et al. 2009). The extent of infection and the presence of abscess formation are best assessed with fat-suppressed T2-weighted, STIR, and post-gadolinium fat-suppressed T1-weighted images (Averill et al. 2009).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


