Chapter 580 Hypofunction of the Ovaries
Hypofunction of the ovaries can be either primary or central in etiology. It may be caused by congenital failure of development, postnatal destruction (primary or hypergonadotropic hypogonadism), or lack of central stimulation by the pituitary and/or hypothalamus (secondary or tertiary hypogonadotropic hypogonadism). Primary ovarian insufficiency (hypergonadotropic hypogonadism), which is also termed premature ovarian failure, is characterized by the arrest of normal ovarian function before the age of 40 yr. Mutations of certain genes could result in primary ovarian insufficiency. Hypofunction of the ovaries due to lack of central stimulation (hypogonadotropic hypogonadism) can be associated with other processes such as multiple pituitary hormone deficiencies and some chronic diseases. Table 580-1 details the etiologic classification of ovarian hypofunction.
Table 580-1 ETIOLOGIC CLASSIFICATION OF OVARIAN HYPOFUNCTION
HYPOGONADOTROPIC HYPOGONADISM
HYPERGONDADOTROPIC HYPOGONADISM
580.1 Hypergonadotropic Hypogonadism in the Female (Primary Hypogonadism)
Turner Syndrome
Turner described a syndrome consisting of sexual infantilism, webbed neck, and cubitus valgus in adult females (Chapter 76). Ullrich described an 8 yr old girl with short stature and many of the same phenotypic features. The term Ullrich-Turner syndrome is frequently used in Europe but rarely used in the USA. The condition is defined as the combination of the characteristic phenotypic features accompanied by complete or partial absence of the second X chromosome with or without mosaicism.
Clinical Manifestations
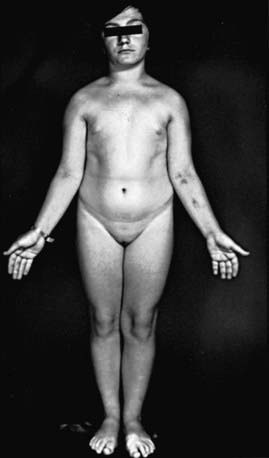
Many patients with Turner syndrome are recognizable at birth because of a characteristic edema of the dorsa of the hands and feet and loose skinfolds at the nape of the neck. Low birthweight and decreased length are common (Chapter 76). Clinical manifestations in childhood include webbing of the neck, a low posterior hairline, small mandible, prominent ears, epicanthal folds, high arched palate, a broad chest presenting the illusion of widely spaced nipples, cubitus valgus, and hyperconvex fingernails. The diagnosis is often first suspected at puberty when breast development fails to occur.
Short stature, the cardinal finding in virtually all girls with Turner syndrome, may be present with little in the way of other clinical manifestations. The linear growth deceleration begins in infancy and young childhood, gets progressively more pronounced in later childhood and adolescence, and results in significant adult short stature. Sexual maturation fails to occur at the expected age. Among untreated patients with Turner syndrome, the mean adult height is 143-144 cm in the USA and most of northern Europe, but 140 cm in Argentina and 147 cm in Scandinavia (Fig. 580-1). The height is well correlated with the midparental height (average of the parents’ heights). Specific growth curves for height have been developed for girls with Turner syndrome.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


