Gestational Trophoblastic Disease: Molar Pregnancy and Gestational Trophoblastic Neoplasia
JULIA N C. SCHINK  JOHN R. LURAIN
JOHN R. LURAIN
Gestational trophoblastic disease (GTD) describes a continuum of interrelated lesions that arise from abnormal proliferation of placental trophoblasts, ranging from benign hydatidiform mole to invasive mole, malignant choriocarcinoma (CCA), and placental site trophoblastic tumor (PSTT) (Table 27.1). Hydatidiform moles, both complete and partial, are benign lesions that resolve following uterine evacuation in the vast majority of cases. Persistent GTD refers to disease that does not resolve after molar evacuation or that becomes malignant and requires active management. Invasive moles, CCA, and PSTT, as well as a variant of PSTT called epithelioid trophoblastic tumor (ETT), are collectively referred to as gestational trophoblastic neoplasia (GTN), with varying degrees of malignant potential. GTN most commonly arises after a molar pregnancy, though it can develop after any pregnancy. Historically, GTD was associated with high rates of morbidity and mortality. Hydatidiform mole was associated with serious complications, and the mortality rate for invasive mole approached 15%. The mortality rate for CCA was near 100% if metastatic disease was present and 60% for nonmetastatic disease even if hysterectomy was performed. Earlier detection with ultrasonography, the use of human chorionic gonadotropin (hCG) as a disease-specific biomarker, advances in uterine evacuation, and the introduction of chemotherapy into the management of GTN (1) have significantly decreased the risk of death associated with GTD and have allowed many women to preserve their fertility after treatment. This chapter will describe the epidemiology and pathology of molar pregnancy and GTN and will discuss the changes in diagnosis and management that have transformed GTN from one of the most deadly to one of the most curable solid tumors in women, with cure rates higher than 90%, even in the presence of metastasis (2,3).
EPIDEMIOLOGY
Epidemiologic data for GTD are unreliable, primarily due to inconsistent case definitions, no centralized databases, and the rarity of certain forms of the disease. Similarly, defining the risk factors that contribute to the development of GTD has been challenging, with an inability to adequately identify at-risk populations and a lack of control groups (4). Based on available data, hydatidiform mole develops in women during their reproductive years (5), with an incidence that varies widely across different geographical regions. In North America, Australia, New Zealand, and Europe, the incidence of molar pregnancy has been reported as 0.6 to 1.1 per 1,000 pregnancies, but it is 2- to 3-fold higher in Southeast Asia and Japan (2.0 per 1,000 pregnancies) (6–8). In Taiwan, hydatidiform mole occurs in 1 in 125 pregnancies, whereas the incidence in the United States is approximately 1 in 1,500 pregnancies. In a study from Ireland, the incidence of complete and partial mole was reported as 1 in 1,945 and 1 in 695 pregnancies, respectively (9).
Despite this geographical variation, the risk of hydatidiform mole has not been linked to any specific ethnic or racial differences, cultural factors, or differences in reporting of hospital-based and population-based data (10–12). However, several studies have reported a link between molar pregnancy and socioeconomic and dietary factors, specifically, that the risk of complete molar pregnancy increases with decreased consumption of vitamin A (carotene) and animal fat (13,14). Regions with a higher incidence of vitamin A deficiency also have a higher incidence of molar pregnancy. A history of infertility is also associated with increased risk of complete and partial mole (15), and a history of spontaneous abortion increases the risk of both complete and partial moles 2- to 3-fold compared with women without a history of miscarriage (15–17).
The two strongest risk factors for complete hydatidiform mole are maternal age and prior molar pregnancy (17). Both very young women and women over the age of 40 have a higher risk of complete molar pregnancy, with older women having a 5- to 10-fold higher risk (18,19). In women over the age of 50, 1 in every 3 pregnancies is molar (4). These observations suggest that the ova of older women are predisposed to the abnormal fertilization events that lead to hydatidiform mole. The risk of a second complete molar pregnancy is 1%, approximately 10- to 20-fold higher than the risk of molar pregnancy in the general population (20,21), and the risk of a third mole is 15% to 20% (22,23), regardless of a change in partner (24).
Familial repetitive hydatidiform mole (17) has been linked to a missense mutation in the NLRP7 locus (25,26) on chromosome 19 (27); in one report, this mutation was present in 60% of patients who had two molar pregnancies (28). The mutated gene is involved in maternal imprinting (29) and is seen in familial clusters of complete moles of biparental origin rather than androgenetic origin (26,30).
There is less information regarding the epidemiology of partial molar pregnancy, though it is clear that it differs from that of complete molar pregnancy (18,19). Partial mole does not appear to be linked to vitamin A deficiency (31) or advanced maternal age (17), but is associated with a history of irregular menstruation and use of high estrogen-containing oral contraceptives (31).
Locally invasive GTN develops in approximately 15% of patients after molar evacuation. CCA occurs in 1 in 50,000 pregnancies (including term, miscarriage, abortion, or ectopic) (32). CCA is 1,000 times more likely to develop after a complete molar pregnancy than after other pregnancy events, with half of all CCA cases arising from molar pregnancies. The risk of CCA increases in women with advanced maternal age and prior hydatidiform mole, and is higher in women of Asian, American Indian, and African American descent (12). Menarche after age 12, light menstrual flow, and long-term use of oral contraceptives are also associated with a higher risk of CCA (33), though the association between postmolar GTN and oral contraceptive use is not entirely clear (34,35). Women with type A blood also have an increased risk of CCA (7,36).
National Institutes of Health Clinical Classification of Gestational Trophoblastic Disease |
I. Benign GTD
A. Complete hydatiform mole
B. Partial hydatidiform mole
II. Malignant GTD
A. Nonmetastatic (invasive mole or CCA)
B. Metastatic
1. CCA
2. PSTT
3. ETT
GTD, gestational trophoblastic disease; CCA, choriocarcinoma; PSTT, placental site trophoblastic tumor; ETT, epithelioid trophoblastic tumor.
PSTT and ETT are extremely rare forms of malignant GTD, and there are insufficient data to characterize the epidemiology or risk factors. Approximately 95% of PSTT and ETT lesions develop after a term pregnancy or nonmolar abortion (37), often several months or even years later.
PATHOLOGY AND CHROMOSOMAL FEATURES
Trophoblastic Differentiation and GTD
Molar pregnancies and GTN originate from the placental trophoblast, which is derived from the outermost layer of the blastocyst, called the trophectoderm (38). The trophoblast is composed of cytotrophoblast, syncytiotrophoblast, and intermediate trophoblast. Syncytiotrophoblast invades the endometrial stroma upon implantation of the blastocyst and secretes hCG and other proteins to regulate the implantation site microenvironment. Cytotrophoblast fuses with syncytiotrophoblast to form the chorionic villi that cover the chorionic sac. Nonvillous cytotrophoblast differentiates into intermediate trophoblast, categorized as either implantation site or chorion type. Implantation site intermediate trophoblast loses the ability to proliferate but invades the maternal decidua and myometrium in a highly controlled manner, migrating to the maternal spiral arteries to facilitate oxygen and waste transfer between the fetus and the mother (Fig. 27.1).
Invasion of healthy trophoblast into the maternal endometrium is a normal, tightly regulated event in pregnancy that is required for the vascular connection between the fetus and the mother. When regulatory mechanisms are impaired, invasive and vascular tumors arise. For example, recent work has described an inhibitory effect of TGF-β and a proteoglycan, decorin, on nonvillous trophoblast cell growth, migration, and invasion, and this negative regulation is lost in trophoblast lesions (39,40).
Most GTD lesions (except partial mole) derive from the fetus and not from the mother, and therefore contain only paternal genetic material (38). A large body of work on the immunobiology of GTD has suggested that a maternal immunologic response is activated by paternal antigens in the trophoblastic cells of GTD lesions, thereby promoting their regression and sensitizing them to chemotherapy; conversely, women with persistent GTD or aggressive disease may have greater histocompatibility such that the paternal antigens do not elicit a strong immune response from the mother (41).
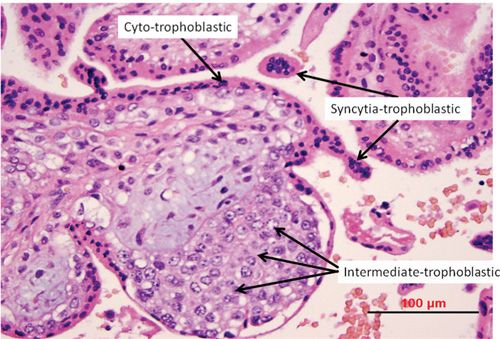
FIGURE 27.1. Normal trophoblast differentiation. Cytotrophoblast, syncytiotrophoblast and intermediate trophoblast are labeled in this photomicrograph.
Immunohistochemical Markers for Differential Diagnosis of GTD |
Marker | Application |
Ki-67, PCNA, p53 | Spontaneous abortion (negative) |
| GTD (positive) |
| CCA (diffusely positive in 50% cells) |
| PSTT (>10% labeling index) |
p63 | PSTT (negative) |
| ETT (positive) |
HLA-G | Nonvillous IT (positive) |
| PSTT (implantation site IT positive) |
| ETT (chorionic-type IT positive) |
β-hCG | CCA (syncytiotrophoblast positive) |
Inhibin α | CCA (trophoblast and IT positive) |
| PSTT (diffusely positive) |
| ETT (diffusely positive) |
hPL | CCA (IT positive) |
| PSTT (diffusely positive) |
Mel-CAM | PSTT (diffusely positive) |
Cytokeratin | CCA (all cells positive) |
| PSTT (diffusely positive) |
| ETT (diffusely positive) |
p57kip2 | Complete mole (negative) |
| Partial mole (positive) |
Cyclin E | ETT (relatively greater staining than placental site nodule) |
PCNA, proliferating cell nuclear antigen; GTD, gestational trophoblastic disease; CCA, choriocarcinoma; PSTT, placental site trophoblastic tumor; ETT, epithelioid trophoblastic tumor; IT, intermediate trophoblast.
All three types of trophoblast can proliferate to produce GTD lesions (42), and each type expresses different antigens that have been useful in the immunohistochemical analysis and differential diagnosis of trophoblastic lesions (43); they may also provide insight into the pathogenic mechanisms underlying GTN (Table 27.2). Expression of Ki67, proliferating cell nuclear antigen, and p53 are significantly higher in GTD compared with normal tissues and can differentiate between GTD and spontaneous abortion (44). p63 isoforms are differentially expressed in cytotrophoblast and intermediate trophoblast (45) and may be useful in differentiating between PSTT (p63 negative) and ETT (p63 positive). HLA-G is also expressed in intermediate trophoblasts but not in villous cytotrophoblasts or syncytiotropho-blasts, and may be useful in the diagnosis of various GTD lesions (46). Several growth factors and oncogenes are abnormally expressed in molar tissues and CCA (15,47,48). Both complete mole and CCA overexpress c-myc, c-erb2, and bcl-2. Epidermal growth factor receptor (EGFR) was found to be more highly expressed in CCA and complete moles compared with normal placenta and partial moles, suggesting that EGF family members may be involved in GTN pathogenesis (49). In addition, there is increased expression of matrix metalloproteinase (MMP-1 and MMP-2) and decreased expression of tissue inhibitor of metalloproteinase (TIMP)-1 in CCA compared with either hydatidiform mole or normal placenta, implicating the dysregulation of extracellular matrix (ECM) in the invasion and metastasis of CCA (50). Characterizing the molecular pathogenesis of GTD is an active area of research that may reveal new diagnostic and prognostic markers, as well as lead to targeted therapies.
Hydatidiform Mole
Molar pregnancies arise from the proliferation of villous cytotrophoblast and syncytiotrophoblast, which produces lesions on the maternal decidua (51,52). A comparison of the characteristics and cytogenetics of complete and partial moles is provided in Table 27.3. Complete hydatidiform moles show early uniform enlargement of villi with hyperplastic and atypical trophoblast and do not contain a fetus/embryo or villous capillaries (Fig. 27.2). Most complete moles (approximately 90%) are 46,XX and arise from the fertilization of an “empty” anucleated egg—missing the pronucleus and maternal chromosomes—by a single sperm followed by duplication of paternal haploid chromosomes (Fig. 27.3) (53,54). The other 10% of complete moles are either 46,XY or 46,XX and are produced by dispermic fertilization of an anucleated egg. Some complete moles can also arise from the loss of maternal chromosomes during the first cleavage. Regardless of monospermic or dispermic fertilization, complete moles contain only paternal chromosomes (androgenetic), though maternal DNA is present in the mitochondria of the egg (55). The presence of excess paternal material leads to trophoblastic hyperplasia, with no formation of a fetus due to the absence of maternal chromosomal DNA. Loss of maternally imprinted genes and extra paternally imprinted genes may also inhibit embryo formation (56).
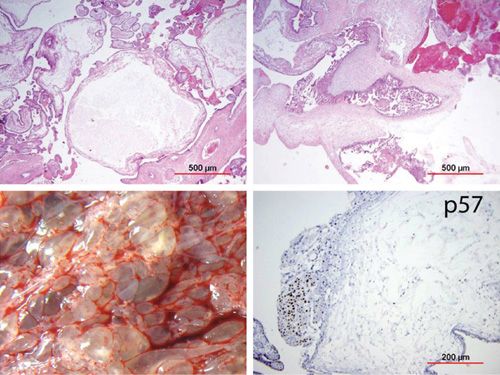
FIGURE 27.2. Complete hydatidiform mole. Upper left: large round chorionic villi with cistern formation; Upper right: large irregular contour with extensive trophoblastic proliferation; Lower left: gross morphology of large cystic chorionic villi; Lower right: chorionic villous stromal cells stain negative for p57.
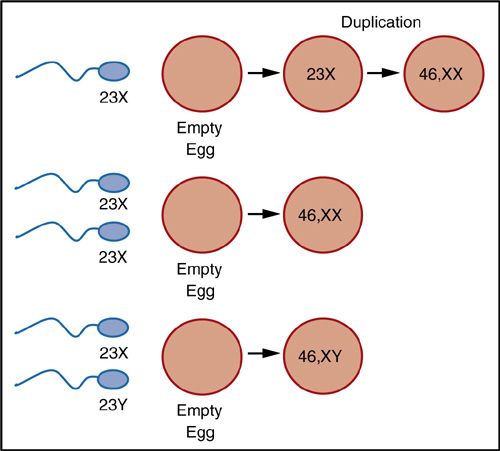
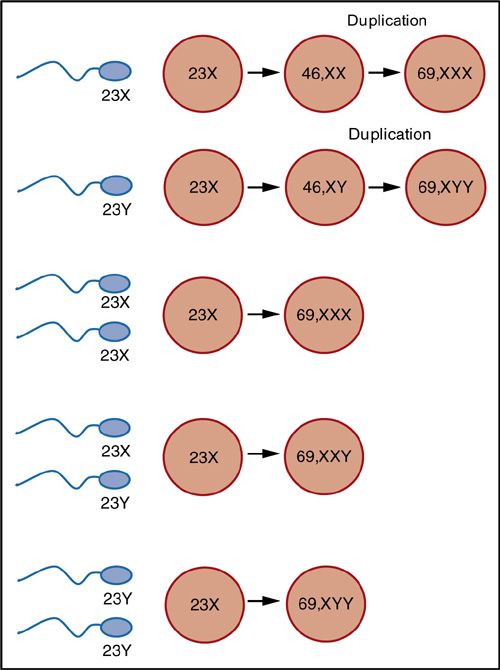
FIGURE 27.3. Karyotypes of complete and partial hydatidiform mole. (A) Complete moles arise from the fertilization of an empty egg with a single sperm that then undergoes duplication (46,XX) or the fertilization of an empty egg with two sperm (46,XX or 46,XY). Complete moles therefore contain only paternal genetic material. (B) Partial moles are triploid (69,XXY; 69XYY; or 69XXX) and arise from either dispermic fertilization of a normal egg or duplication of chromosomes in a single sperm after fertilization of a normal egg.
In contrast, partial hydatidiform moles contain fetal/embryonic tissue, and the chorionic villi show varying degrees of focal enlargement and edema, predominantly syncytiotrophoblast hyperplasia, scalloping of the villous outline, prominent stromal inclusions, and functional villous circulation (Fig. 27.4) (57). Like incomplete moles, the trophoblast is hyperplastic but shows only mild atypia. In later stages of partial molar pregnancy, the fetus shows congenital abnormalities, such as syndactyly of the fingers and toes (57). The majority of partial moles are triploid, most often 69,XXY, with two sets of paternal chromosomes as a consequence of either dispermic fertilization of a normal egg or duplication of chromosomes in a single sperm after fertilization of a normal egg (Fig. 27.3) (51,56,58).
Invasive Mole
Invasive mole is a condition in which hydatidiform mole, with hydropic villi and proliferating trophoblast, has invaded the myometrium through the tissue or veins (Fig. 27.5). Molar villi may be observed on the uterine serosa, and extrauterine tubal and ovarian moles can occur (59). Invasive moles are less hydropic, and trophoblastic proliferation is easily seen (Table 27.3) (57).
Choriocarcinoma
Approximately 2% of women with complete moles may develop CCA, characterized by a mixture of cytotrophoblast and syncytiotrophoblast hyperplasia, hemorrhage, and necrosis, and the absence of chorionic villi (Fig. 27.6) (57). Direct invasion of the myometrium and vasculature is also present, which permits metastasis to the lungs, brain, liver, pelvis and vagina, kidney, intestines, and spleen. Immunohistochemical markers can confirm a histologic diagnosis of CCA, with tumors staining strongly for hCG and inhibin α in the trophoblast, human placental lactogen (hPL) and inhibin α in intermediate trophoblast, and cytokeratin in all trophoblast cells (Tables 27.2 and 27.3) (60). Ki-67 is diffusely expressed in approximately half of the cells (61).
Placental Site Trophoblastic Tumor
PSTT lesions are usually diploid and monomorphic, developing from placental implantation site intermediate trophoblast after a normal or aborted uterine pregnancy (62). PSTT lesions contain primarily mononuclear intermediate trophoblast without chorionic villi that infiltrates the uterine wall in sheets or cords between myometrial fibers (Fig. 27.7). Compared with CCA, there is less hemorrhage, necrosis, and vascular invasion, but there is a higher risk of lymphatic metastasis. hCG production is focal, leading to relatively lower serum levels (Table 27.3). These tumors may be diagnosed immunohistochemically, and contain diffuse cytokeratin and human placental lactogen (63), as well as inhibin α (60) and Mel-CAM (Table 27.2) (61). The Ki-67 labeling index is also usually elevated (>10%) in a neoplastic lesion of nonvillous trophoblast (61).
Epithelioid Trophoblastic Tumor
Epithelioid trophoblastic tumor (ETT) is a rare malignant tumor that arises from neoplastic transformation of chorion-type intermediate trophoblast (62). These lesions appear as nodules of mononuclear intermediate trophoblast, surrounded by hyalinized extracellular matrix within extensive necrotic tissue and with preserved blood vessel structure (Fig. 27.8 and Table 27.3). Intratumor hemorrhage and metastases are rarely observed. ETT tumor cells show diffuse expression of immunohistologic markers, including cytokeratin and inhibin α (Table 27.2) (64). Cyclin E staining is higher in ETT than placental site nodule and can help in differentiating between the two (64–66).
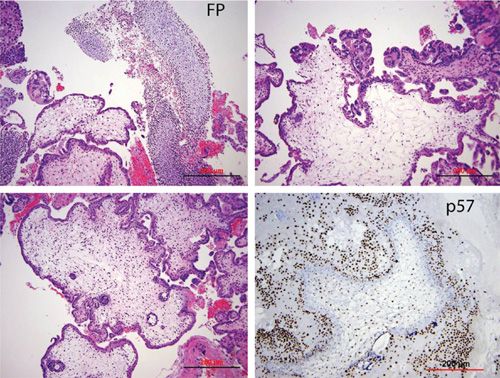
FIGURE 27.4. Partial hydatidiform mole. Upper left: large chorionic villi and fetal parts (FP); Upper right: large irregular contour and trophoblastic proliferation; lower left: large irregular contour with pseudoinclusion cysts; lower right: chorionic villous stromal cells stain positive for p57.
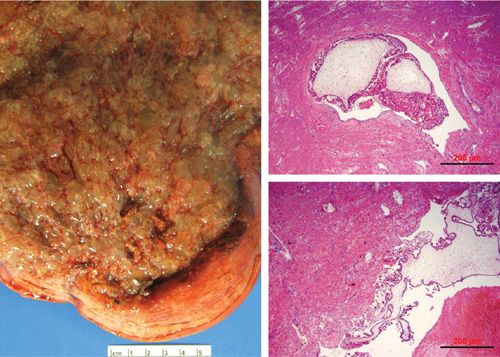
FIGURE 27.5. Invasive mole. Macrophotograph of molar product of conception that is occupying the entire endometrial cavity and invading into the myometrium (left panel). Photomicrographs show molar chorionic villi infiltrating into the myometrium (right panels).
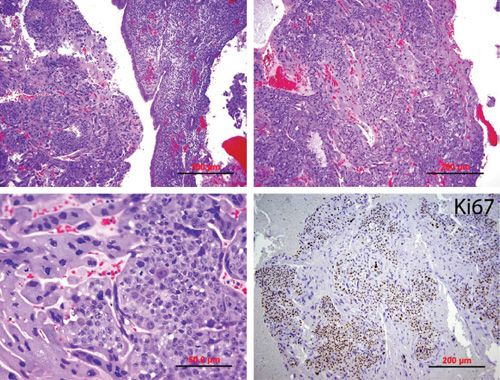
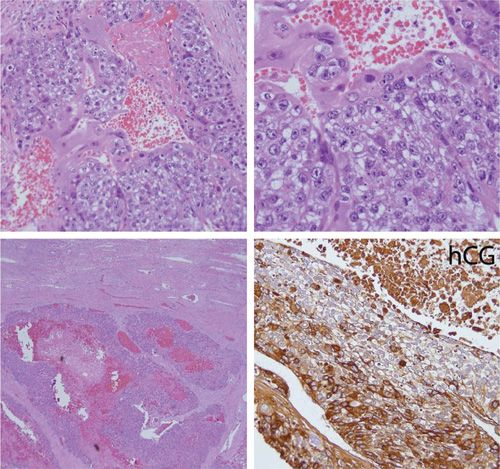
FIGURE 27.6. Choriocarcinoma. (A) Upper left: fragment of trophoblastic proliferation in the background of normal appearing endometrium; Upper right: sheath of cyto- and syncytiotrophoblastic proliferation with hemorrhage; Lower left: close view of biphasic cytotrophoblastic and syncytiotrophoblast cell proliferation; Lower right: Ki-67 index is >50% in tumor cells. (B) Upper panels: close view of biphasic cyto- and syncytiotrophoblastic proliferation; Lower left: tumor invasion into myometrium with characteristic hemorrhage; Lower right: immunostain for hCG is positive in most syncytiotrophoblast cells.
Clinicopathologic Features of Gestational Trophoblastic Diseases |
Disease | Pathologic Features | Clinical Features |
Complete mole | • Diploid (46,XX and some 46,XY) • No fetus or embryo • Diffuse swelling of villi • Diffuse trophoblastic hyperplasia | • Vaginal bleeding • Large for date uterine size • Bilateral theca lutein cysts • hCG can be >100,000 mIU/mL |
Partial mole | • Triploid (69,XXY; 69,XYY; 69,XXX) • Abnormal fetus or embryo • Focal swelling of villi • Focal trophoblastic hyperplasia with mild atypia | • Symptoms of incomplete or missed abortion • Vaginal bleeding • hCG rarely elevated>100,000 mIU/mL |
Invasive mole | • Trophoblastic hyperplasia • Swollen villi • Myometrial invasion | • Irregular postmolar vaginal bleeding • Persistent hCG elevation • 15% symptoms of lung/vaginal metastases |
Choriocarcinoma | • Mixture of cytotrophoblast and syncytiotrophoblast hyperplasia • No villi • Myometrial invasion and metastatic potential • Hemorrhage • Necrosis | • Irregular postmolar vaginal bleeding • Persistent hCG elevation • Metastases and associated symptoms |
PSTT | • Diploid • IT hyperplasia • No villi • Less hemorrhage and necrosis • High potential for lymphatic invasion and metastasis • Focal hCG production | • Low serum hCG • Enlarged uterus • hCG levels normal to 1,000 mIU/mL • Metastases and associated symptoms |
ETT | • IT nodules surrounded by hyalinized ECM • Extensive necrotic tissue • Preserved blood vessel structure • Hemorrhage and metastases rare |
|
hCG, human chorionic gonadotropin; IT, intermediate trophoblast; ECM, extracellular matrix; PSTT, placental site trophoblastic tumor; ETT, epithelioid trophoblastic tumor.
Source: Adapted from Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obstet Gynecol. 2010;203(6):531–539, with permission.
The Changing Clinical Signs of Molar Pregnancy |
Clinical Sign | Incidence (%) | |
| 1970s | 2010s |
Vaginal bleeding | 100 | 90 |
Uterine enlargement | 54 | 28 |
Toxemia | 22 | 1 |
Hyperemesis | 28 | 8 |
Hyperthyroidism | 10 | <1 |
Trophoblastic emboli | 2 | <1 |
Bilaterally enlarged ovaries | 15 | 15 |
Absence of fetal heart sounds | 100 | 100 |
MANAGEMENT OF MOLAR PREGNANCY
Clinical Presentation
Approximately 80% to 90% of women with complete hydatidiform mole present with vaginal bleeding, occurring at 6 to 16 weeks gestation. Women may also present with larger uterine size than expected for gestational date, toxemia, hyperemesis, and hyperthyroidism in the first or second trimester. However, the widespread use of ultrasonography in developed countries and accurate hCG tests to evaluate vaginal bleeding have led to earlier diagnosis of molar pregnancy, and other clinical signs and symptoms are seen less often (Table 27.4) (67). hCG levels can be greater than 100,000 mIU/mL in a complete molar pregnancy, and there are no fetal heart tones (Table 27.3); however, hCG levels vary widely in individual patients, and with earlier ultrasound detection, patients may not present with extremely elevated hCG. It should also be emphasized that a high hCG level alone is not sufficient for a diagnosis of hydatidiform mole, and a confirmatory ultrasound should be performed. In approximately 15% of women with complete hydatidiform mole, ultrasound imaging reveals the presence of bilateral theca lutein cyst enlargement of the ovaries (5,67–69).
Partial hydatidiform mole presents quite differently from complete mole. The vast majority of patients—greater than 90%—present with symptoms of incomplete or missed abortion. Vaginal bleeding occurs in 75% of patients with a partial molar pregnancy, and uterine enlargement, hyperemesis, hypertension, hyperthyroidism, and theca lutein cysts are not often seen. Presenting hCG levels are higher than 100,000 mIU/mL in only 10% of patients (70–72).
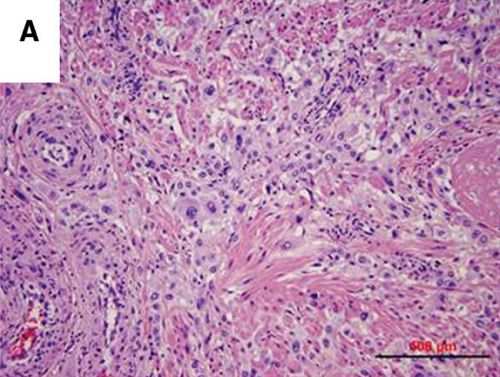
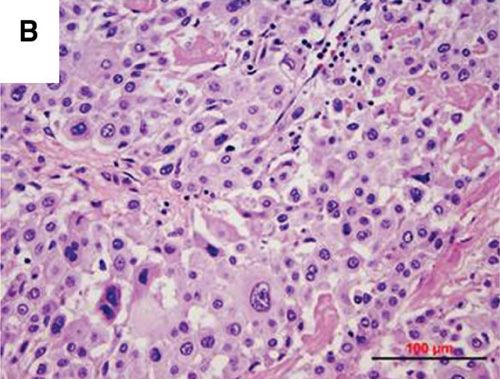
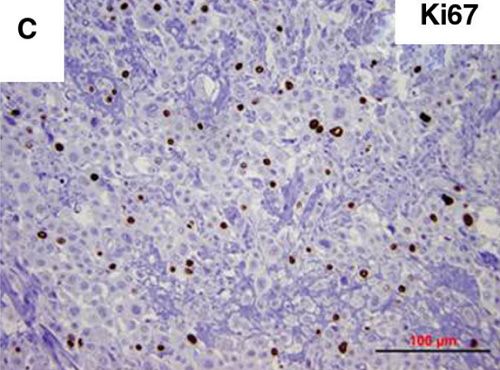
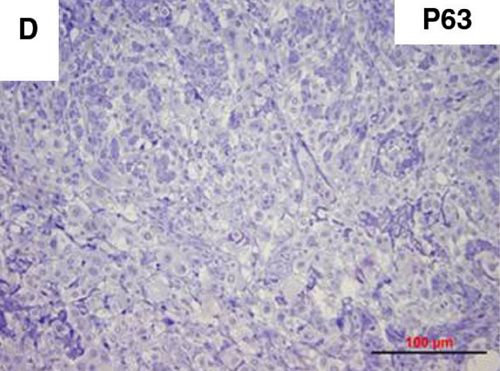
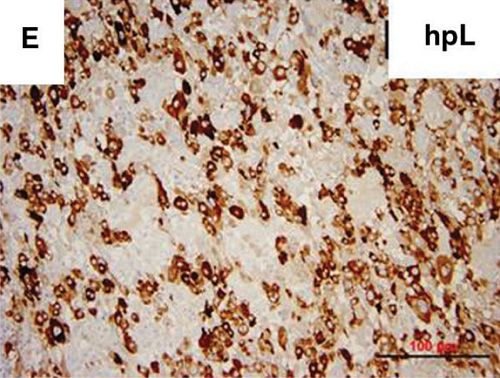
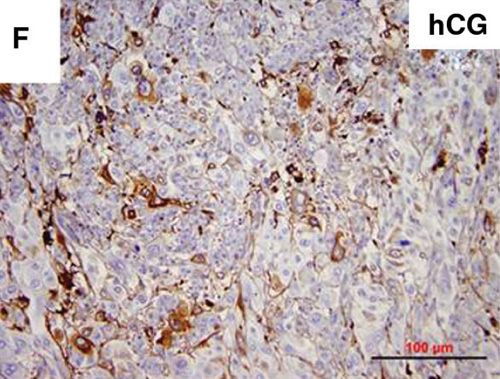
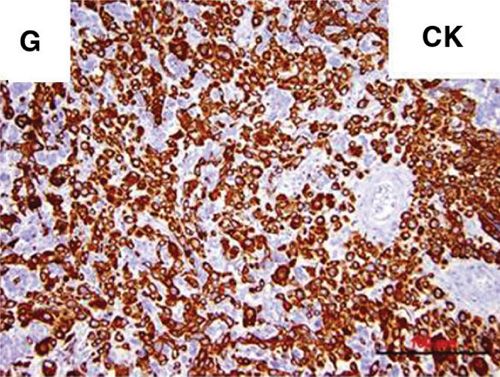
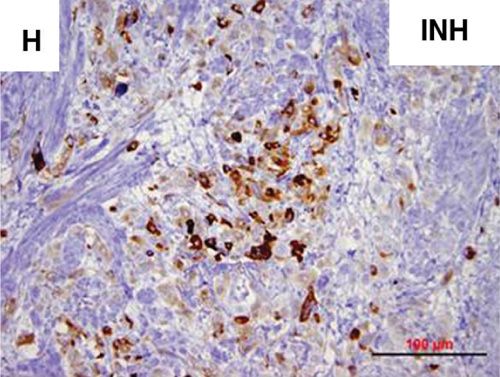
FIGURE 27.7. Placental site trophoblastic tumor (PSTT). (A, B) Histology shows mostly intermediate placental site trophoblastic cell proliferation and infiltration into the myometrium. (C) Tumor cells show moderate cytologic atypia and have an increased Ki-67 index (>20%). Tumor cells are also negative for p63 (D), which excludes a diagnosis of epithelioid trophoblastic tumor; are strongly and diffusely positive for human placental lactogen (E) and pan-cytokeratin (G); and are diffusely positive for hCG (F) and inhibin (H). CK, cytokeratin; hPL, human placental lactogen; INH, inhibin.
Diagnosis
Ultrasonography is the primary means of preoperative diagnosis of molar pregnancy, and its introduction has made diagnosis at much earlier stages possible (5,73–75). Ultrasound not only provides information on the type of molar pregnancy, but also determines involvement of the endometrial cavity or myometrium, assesses the risk of uterine perforation, and detects theca lutein cysts and vaginal metastases. The diffuse hydropic swelling of the chorionic villi in complete molar pregnancy is seen as a characteristic vesicular “snowstorm” pattern on ultrasound, with many holes within the placenta and the absence of a fetus (Fig. 27.9). However, as this pattern is also seen in women with missed abortion, hematometra, or uterine fibroids ultrasound diagnosis alone is not very specific. When ultrasound diagnosis is combined with elevated hCG and the absence of fetal heartbeat, molar pregnancy is the most likely diagnosis. For partial moles, ultrasonography can detect focal cystic spaces in the placental and the enlarged gestational sac (75). Ultrasound may show the snowstorm pattern and a viable fetus, which may also indicate threatened abortion, fibroid uterus, or twin gestation with a single missed abortion and a complete mole. Partial mole can be confirmed with chorionic villus sampling that shows triploidy.
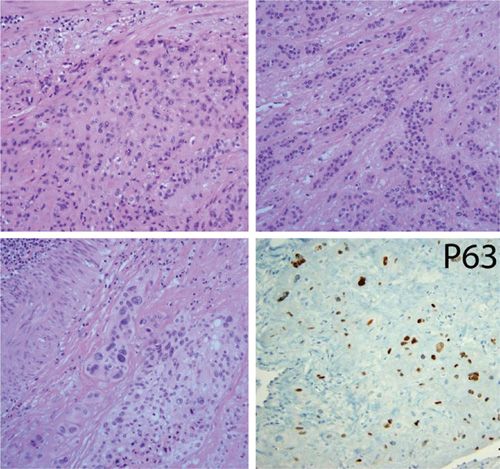
FIGURE 27.8. Epithelioid trophoblastic tumor. Tumor cell proliferation in sheets (upper left) or cords (upper right), and myometrial invasion (lower left). Tumor cells stain positive for p63.
The most accurate disease-specific marker of GTD is hCG, which is produced by hydatidiform moles and CCA and can be measured quantitatively in the blood and urine. Placental hCG is a glycoprotein of two subunits, a common α subunit that is similar to the α subunit of pituitary hCG and a placenta-specific β subunit. In a normal pregnancy, hCG is essential for maintaining placental vascular supply (76). As pregnancy progresses, hCG is secreted by syncytiotrophoblasts, increasing to approximately 60,000 mIU/mL at 10 weeks and then declining to a range of values around 12,000 mIU/mL through the remainder of the pregnancy (77). hCG molecules secreted by trophoblast-derived moles and GTN are more heterogenous than in a normal pregnancy, with transformation of the trophoblast resulting in fragmentation of the hCG molecule, and several forms of hCG are present, including hyperglycosylated, nicked, C-terminal truncated β subunit, free β subunit, nicked free β subunit, and free α subunit (78). Normally, hyperglycosylated hCG is produced by cytotrophoblasts early in gestation and acts as an autocrine regulator of trophoblast invasion of the implantation site and establishment of the fetomaternal circulation. Hyperglycosylated β subunit is produced by GTN lesions and promotes the growth and invasion of the malignant trophoblasts (79).
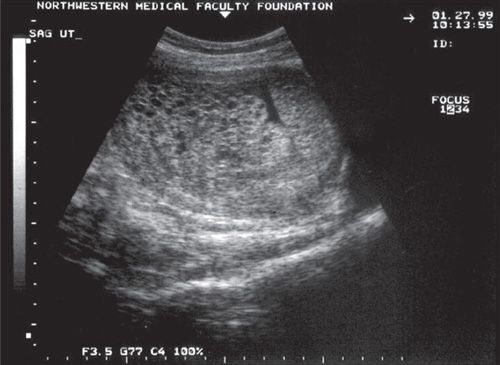
FIGURE 27.9. Ultrasound of complete hydatidiform mole. The characteristic vesicular “snowstorm” pattern of multiple echoes, appearing as holes within the placenta. No fetus is present.
It is, therefore, essential that quantitative assays used to diagnose or follow up GTD detect all forms of the hCG protein and its degradation products. In one study, Cole et al., compared several commercially available hCG tests and found significant variations in assay results related to differences in recognition of hCG variants (80). The most common hCG assay is a monoclonal antibody sandwich assay (81). Complete hydatidiform moles present with markedly elevated hCG, with half of patients having levels greater than 100,000 mIU/mL (82,83). Because hCG levels in a normal pregnancy are highest at the end of the first trimester, hCG measurements need to be taken at several times to differentiate a complete molar pregnancy from a normal gestation, multiple gestation, or pregnancy complicated by diseases that are associated with an enlarged placenta. By contrast, hCG levels greater than 100,000 mIU/mL are seen in only 10% of patients with partial moles (71,72).
Diagnosis of complete and partial moles may also include pathologic examination of curettage tissue; however, with the diagnosis of hydatidiform mole occurring earlier in gestation, histologic analysis can be challenging (84,85). Cytogenetic analysis can differentiate between complete mole (androgenetic diploidy), partial mole (diandritic triploidy), and hydropic abortus (biparental diploidy). A hydropic abortus can contain enlarged villi, but lacks proliferating trophoblast (57). Immunohistochemical analysis may also help to confirm a diagnosis of molar pregnancy; specifically, p57kip2 expression can differentiate between complete and partial hydatidiform moles (Table 27.2) (86–90). This protein is paternally imprinted and maternally expressed; therefore, the villous cytotrophoblast cells in complete moles, which lack maternal chromosomes, will stain negative for p57kip2, whereas partial moles and hydropic abortus will stain positive. Fluorescence in situ hybridization can be used to distinguish between p57kip2-positive partial moles (triploid) and hydropic abortus (diploid) (91). PHLDA2 is another maternally imprinted gene that can be used to identify partial moles (92).
False-Positive hCG Tests
hCG measurements are a critical diagnostic tool for GTD, but some assays may produce false-positive or “phantom” hCG results (93). False-positive hCG tests, some as high as 800 mIU/mL, can lead to unnecessary surgery and chemotherapy in healthy patients (94). These false-positive results are due to the presence of nonspecific heterophilic antibodies that mimic hCG and can interfere with the hCG sandwich assay. These antibodies are present in 3% to 4% of healthy people. Because the antibody does not pass into the urine, false-positive hCG test results can be identified by determining hCG levels in the urine. In addition, serial dilution of the serum sample would not show a decrease in the detected antibody.
Luteinizing hormone (LH) can also cross-react with hCG assays, leading to falsely elevated hCG in women with elevated pituitary FSH, LH, or hCG. hCG normally increases with age, and perimenopausal and postmenopausal women may have low-level hCG test results. To determine whether the hCG detected in the serum is from the pituitary, women may be given oral contraceptive to suppress LH, followed by simultaneous measurement of LH and hCG (95,96).
Treatment
Suction evacuation and curettage is the preferred treatment for hydatidiform mole in patients who wish to preserve their fertility (Table 27.5) (97,98). Patients should undergo a preoperative evaluation including vital signs, laboratory tests, and electrocardiogram to identify any medical complications, such as anemia, preeclampsia, and hyperthyroidism. The patient’s blood type and hCG levels should also be measured preoperatively. If the patient is hemodynamically stable, the type of molar evacuation procedure can be selected (99,100). If the uterus is greater than 12-week size, ultrasound monitoring should be used to prevent uterine perforation and ensure complete removal of the molar tissue. Suction evacuation and curettage is performed under anesthesia, and the cervix is dilated to allow passage of a 12- to 14-mm suction cannula into the lower uterine segment. The cannula is rotated to remove the intrauterine contents. Intravenous oxytocin should be started at the onset of the procedure and continued postoperatively for several hours to enhance uterine contraction. Rh-negative patients will also need to receive Rh immuno-globulin during evacuation because the Rh D factor is expressed by trophoblastic cells (99,100). Gentle sharp curettage should be applied after suction evacuation. At least 2 units of blood should be available because of the risk of bleeding, which increases with uterine size. Postoperative respiratory distress may occur due to trophoblastic embolization, excessive fluid resuscitation, or massive oxytocin infusion. Attention to blood and crystalloid replacement reduces the risk of pulmonary complications, though all patients should be monitored with a pulse oximeter for at least 2 hours after surgery. Patient outcomes can be improved with the judicious use of equipment, ready access to blood products, careful monitoring during the procedure, and anticipation and treatment of complications.
For patients who have completed childbearing and do not wish to preserve their fertility, hysterectomy may be performed as an alternative to suction evacuation and curettage (Fig. 27.10). Hysterectomy removes the risk of local myometrial invasion, and focal disease can be ruled out in patients with persistent GTD. The high cost of this procedure and the risk of complications should limit the use of hysterectomy to those patients at high risk of postmolar GTD, including women over the age of 40, greater than gestational date uterine size, theca lutein cysts greater than 6 cm, hCG greater than 100,000 mIU/mL, and medical complications of pregnancy. However, metastatic disease may still be present after hysterectomy, with a 3% to 5% risk of postmolar GTN, and patients should be followed up with serial hCG testing (97).
Evacuation of Hydatidiform Mole |
Preoperative evaluation and preparation
1. Chest X-ray
2. Complete blood count
3. Electrolytes
4. Baseline oxygen saturation
5. Type and cross 2 units of blood
6. Set up Rho (D) immunoglobulin (RhoGAM–) if patient is Rh-negative
Surgical procedure (with ultrasound guidance if uterus is >12 wk size)
1. Premedication and paracervical anesthesia
2. Dilatation
3. Suction curettage—leave cannula at lower uterine segment until majority of molar tissue has been removed
4. Begin intravenous oxytocin infusion
5. Gentle sharp curettage
Postevacuation
1. Monitor respiratory status and uterine bleeding for at least 2 h
2. Give RhoGAM if Rh-negative
3. Prescribe contraceptive
4. Follow hCG levels every 2 wk until 2 consecutive normal results, then every month for 6 mo and every 3 mo twice
hCG, human chorionic gonadotropin.
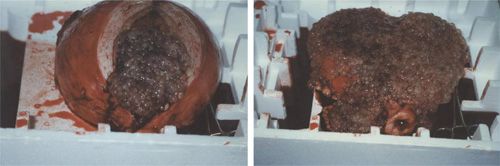
FIGURE 27.10. In selected patients, hysterectomy may decrease the likelihood of postmolar GTN. This photograph shows a 16-week size uterus filled with complete hydatidiform mole.
Medical induction of labor and hysterotomy are not recommended, because of the increased risk of maternal morbidity, including blood loss, incomplete evacuation requiring surgical intervention, and the need for cesarean delivery in subsequent pregnancies. This approach also increases the risk of trophoblastic dissemination and development of postmolar GTN requiring chemotherapy (98).
Use of prophylactic chemotherapy—either methotrexate or actinomycin D—at the time of evacuation or immediately afterwards can reduce the risk of postmolar GTN from 15%–20% to 3%–8%. However, this approach exposes patients to chemotherapeutic toxicity but benefits only a small number of patients. Because all patients who are found to have persistent postmolar GTD with serial hCG testing can be cured with chemotherapy, the use of prophylactic chemotherapy should be limited to those patients who have a greater than normal risk of postmolar GTN or who are less likely to comply with serial hCG testing during follow-up (101–103).
Molar Pregnancy and Coexisting Fetus
Twin pregnancies of a complete mole and normal fetus occur approximately once in every 22,000 to 100,000 pregnancies and may be difficult to distinguish from partial mole. Ultrasound can usually differentiate between these two scenarios, though cytogenetics may help distinguish a normal viable fetus from a triploid nonviable fetus in a partial mole. Patients with a twin normal/complete mole pregnancy are at higher risk of hemorrhage and other complications as well as a higher risk of persistent GTD. Although suction evacuation and curettage are recommended to terminate the pregnancy, 40% of these pregnancies will result in a normal viable fetus if left untreated (104–106).
Follow-Up
Clinical findings of successful evacuation include prompt uterine involution, ovarian cyst regression, and cessation of bleeding. Definitive follow-up after molar evacuation requires serial serum quantitative hCG measurements every 1 to 2 weeks until 3 consecutive normal tests, and then every 3 months for 6 months to 1 year after normalization. More than 50% of patients will achieve a normal hCG within 2 months of evacuation. Contraception is recommended for 6 months after the first normal hCG result so that any postmolar elevation in hCG that is detected can be distinguished from the hCG rise that occurs in a normal pregnancy. Oral contraceptives are preferred because they suppress LH and remove any interference with hCG assay measurements. Studies have shown that oral contraceptives do not increase the risk of postmolar GTN (107–109).
Prognosis
Disease-free survival and fertility is achieved in 80% of patients with hydatidiform mole, and compliant patients who are followed closely with serial hCG measurements are more likely to achieve cure. High-risk postmolar disease is more often seen after a term pregnancy or in patients who were lost to followup. There is a 1% to 2% increased risk of developing a second complete molar pregnancy (110), and a much lower risk of a second partial molar pregnancy (111).
Quiescent GTD
Some women with a history of GTD or spontaneous abortion may have a consistently low level of hCG (<200 mIU/mL for at least 3 months) but no detectable disease. There is also no hyperglycosylated hCG, which would indicate cytotrophoblastic invasion. This “quiescent GTD” does not respond to either surgery or chemotherapy. It is believed that the hCG being detected in these patients is produced by dispersed foci or individual slow-growing syncytiotrophoblast cells with no invasive potential in the absence of cytotrophoblast or intermediate trophoblast. Approximately one-quarter of patients with quiescent GTD go on to develop active GTN, with detectable increases in both hCG and hyperglycosylated hCG levels (112,113). These patients may secrete increased hyperglycosylated hCG within 5 years of the initial pregnancy event, weeks to months before a detectable rise in hCG or clinical evidence of GTN (114). To diagnose quiescent GTD, false-positive hCG testing should be ruled out and the patient examined for any evidence of disease. Patients should be monitored closely with periodic hCG testing and should avoid pregnancy (95). Chemotherapy and surgery should be avoided unless a diagnosis of GTN can be made, based on either a sustained rise in hCG or the appearance of disease.
Pregnancy after Hydatidiform Mole
All women with a history of molar pregnancy have a higher risk of developing malignant disease in a subsequent pregnancy. After molar evacuation, women should wait at least 6 months from the time of hCG normalization to become pregnant. For all future pregnancies, pathologic examination of the placenta and other products of conception and measurement of hCG 6-weeks postpartum are recommended.
Persistent GTD/Postmolar GTN
Postmolar invasive mole or CCA occurs after 15% to 20% of complete and 1% to 5% of partial molar pregnancies, and invasive mole is seen more frequently (85% to 90%) than CCA (10% to 15%) (51,52,58,99,115–120). Approximately, half of all cases of CCA arise from a prior molar pregnancy, but only 2% to 3% of all hydatidiform moles will progress to CCA (121). A diagnosis of CCA after a partial mole has been reported as single cases in the literature (51,52,58,122–126). Of those with invasive mole, 15% will have metastatic disease to the lungs or vagina. Most PSTTs and ETTs arise after nonmolar pregnancies, sometimes years after the pregnancy event (64,127,128).
The likelihood of persistent GTD after a molar pregnancy is higher in women who initially presented with marked trophoblastic growth, as indicated by hCG levels greater than 100,000 mIU/mL, excessive uterine size (>20 weeks), and theca lutein cysts greater than 6 cm in diameter. Women who have at least one of these risk factors have a 40% chance of developing postmolar GTN, compared with a 4% risk in those with none of these factors. Other risk factors for postmolar GTN include age greater than 40 years, repeat molar pregnancy, aneuploidy mole, and medical complications of molar pregnancy, such as toxemia, hyperthyroidism, and trophoblastic embolization (99).
At the molecular level, studies have found that women who will develop postmolar disease are more likely to show telomerase activity (129). Conversely, apoptotic activity measured by various techniques is higher in hydatidiform moles that spontaneously regress versus those that go on to develop postmolar GTN (130,131). Other studies have found that hydatidiform moles that are more likely to progress to malignant disease have lower expression of the anti-apoptotic gene Mcl-1 (132), ferritin light polypeptide (FTL), and IGFBP-1 (133).
Repeat curettage for persistent GTD is not recommended, except in patients with excessive uterine bleeding and intracavitary molar tissue on radiologic scans. In one retrospective study, although 9.4% of women who underwent repeat curettage avoided chemotherapy, there was a 2.4% risk of uterine perforation (134). Thus, the small benefit of repeat curettage in achieving remission or improving treatment outcomes does not outweigh the risk of uterine perforation and hemorrhage (134–137). A prospective phase II Gynecologic Oncology Group (GOG) trial is under way that will determine the utility of second curettage and whether benefit and risk vary with the depth of uterine infiltration (GOG 242, NCT00521118).
GESTATIONAL TROPHOBLASTIC NEOPLASIA
Clinical Presentation
The clinical presentation of GTN depends on the pregnancy event, the extent of disease, and histopathology. Postmolar GTN, either invasive mole or CCA, presents as irregular bleeding after evacuation of a hydatidiform mole (usually a complete mole). Invasive mole is diagnosed clinically rather than pathologically, with persistent hCG elevation after molar evacuation. CCA occurs in association with any pregnancy event, with approximately 25% of cases occurring after abortion or tubal pregnancy, 25% after term or preterm gestation, and 50% after a molar pregnancy. Sometimes, a metastatic vaginal lesion may be disrupted during pelvic examination, which can lead to uncontrolled vaginal bleeding. Women with postmolar GTN may also present with an enlarged, irregular uterus and bilateral ovarian enlargement. There are no signs or symptoms that differentiate between postmolar GTN and GTN arising after a nonmolar pregnancy event, as these symptoms are related to the invasion and metastasis of the tumor. GTN should be considered in patients who present with postpartum bleeding and subinvolution, although other causes include endomyometritis, tumors in other organ systems, or another pregnancy. Uterine perforation and metastases can cause abdominal pain, hemoptysis, melena, or increased intracranial pressure that leads to headaches, seizures, or hemiplegia. Symptoms suggesting pulmonary involvement include dyspnea, cough, and chest pain (121), and early respiratory failure requiring mechanical ventilation may develop. A diagnosis of GTN should be considered for any women of reproductive age who presents with pulmonary symptoms. Symptoms of brain metastases include vomiting, seizures, headache, hemiparesis, and speech and visual disturbances. Liver and gastrointestinal metastases are rare, and usually are seen with simultaneous lung or brain involvement; these patients have the lowest survival rate (138). PSTT and ETT often present with irregular vaginal bleeding and an enlarged uterus, with hCG levels from normal to 1,000 mIU/mL, sometimes years after a previous pregnancy. PSTT may also present with liver, lung, or brain metastases, or complications such as neoplastic nephrotic syndrome. The risk of metastatic PSTT is higher in patients with more than 5 mitoses per 10 high-power fields.
Diagnosis
The International Federation of Gynecology and Obstetrics (FIGO) defined a set of criteria for diagnosing persistent GTD in 2002 (Table 27.6) (139). Postmolar GTN is usually diagnosed when hCG levels plateau or rise during follow-up after molar evacuation, without histologic diagnosis. An hCG plateau is defined as a less than 10% decline in 4 measurements taken over 3 weeks. A rise is defined as a greater than 20% increase in 3 measurements taken over 2 weeks. The presence of elevated hCG in addition to metastases usually indicates CCA, whereas with PSTT and ETT, serum hCG levels are only slightly elevated, making differential diagnosis particularly challenging (64,127,128). The free hCG β subunit may be the best biomarker for diagnosing PSTT, and the β core fragment for ETT (38,76). Although a diagnosis of GTN can be confirmed pathologically by examination of the curettage, or hysterectomy specimens, or the placenta, or biopsy of metastatic lesions, the risk of hemorrhage is too high, and biopsy of vaginal lesions should be avoided (140).
For any patient with suspected or established GTN, a metastatic workup and evaluation of risk factors is performed (3,32,110,141). A complete history, physical examination, and laboratory tests (including complete blood cell count, coagulation study, serum chemistries, blood type and antibody screening, and quantitative serum hCG level) should be taken. Radiologic studies should start with a chest X-ray; if abnormal, a CT or MRI of the chest should be performed to detect pulmonary metastases. CT scans of the abdomen and pelvis and MRI of the brain should also be performed. The vast majority of patients with brain involvement (94%) have associated lung metastases; conversely, 20% of patients with lung metastases also have brain metastases. Brain metastases tend to appear in the parietal lobe, and on the right side of the brain (Fig. 27.11). If the physical examination and the chest X-ray are normal and there are no symptoms of metastasis, other sites of metastasis are rarely present. To detect brain involvement, hCG testing of the cerebrospinal fluid (CSF) may be helpful; a serum/CSF hCG ratio of less than 60:1 is a sensitive marker of CNS metastasis (142), although false positives can occur if measurements are taken when hCG levels are falling. Pelvic ultrasound and MRI may be useful to detect extensive uterine disease and identify patients who may benefit from hysterectomy. Biopsy of metastases is not recommended, as the associated risks of biopsy outweigh the benefits of confirming a diagnosis of metastatic disease.
FIGO 2000 Criteria for Diagnosis of Persistent GTD/Postmolar GTN |
hCG plateau lasting for 4 measurements over a period of at least 3 wk (days 1, 7, 14, and 21)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


