Anatomical site
Percentage (%)
Floor of mouth
30
Tongue
26
Oropharynx
17
Anterior neck
13
Epiglottis/Vallecula
9
Retropharynx
4
Approximately 50 % of patients with foregut duplication cysts have no symptoms at presentation. Of those who present with symptoms, the most common presenting clinical features are feeding difficulties, odynophagia, stridor, tongue edema and speech difficulties. The neonate, however, may present with frank respiratory distress secondary to airway obstruction from the mass [6].
Differential Diagnosis
The differential diagnosis of these lesions is that of any congenital cystic mass in the head and neck, the anatomical sub-site indicating a more specific differential . Therefore, the following differential should be considered:
Mucocoele
Rannula
Dermoid
Lymphatic malformation
Venous malformation
Teratoma
Thyroglossal duct cyst
Epidermoid cyst
Lymphoepithelial cyst
Diagnosis and Evaluation
Physical Examination
The commonest site for a foregut duplication cyst to arise is from the floor of mouth or anterior tongue [6]. Such a lesion should be obvious on routine oral cavity examination in the neonatal period (Fig. 19.1).
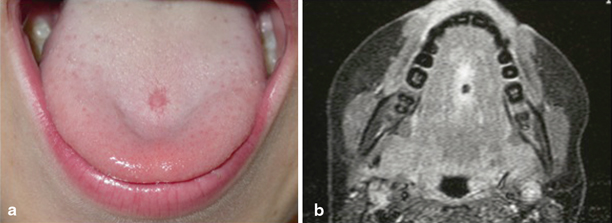
Fig. 19.1
Clinical photograph (a) and MRI (b) from the same patient of a foregut duplication cyst located in the anterior tongue
Those rarer lesions in the oropharynx, hypopharynx and supraglottis are either visible on oral cavity examination, fiberoptic laryngoscopy or at the time of a direct laryngoscopy (being performed for feeding or airway symptoms).
Imaging Evaluation
In evaluating these lesions, imaging (computed tomography, CT, or magnetic resonance imaging, MRI) is invaluable. Although a foregut duplication cyst is indistinguishable from thyroglossal duct cyst and dermoid cyst in terms of appearance on CT and routine MRI pulse sequences, the presence of a cystic mass in the anterior floor of mouth or anterior third of the tongue is suggestive of the diagnosis (Fig. 19.2). Anatomically, thyroglossal duct cysts are usually located between the foramen cecum and hyoid bone or within the infrahyoid neck, whereas vallecular cysts are located between the epiglottis and tongue base in the supraglottic larynx. Mucous retention cyst may, however, appear indistinguishable from foregut duplication cyst in terms of both imaging characteristics and location, especially in the floor of mouth.
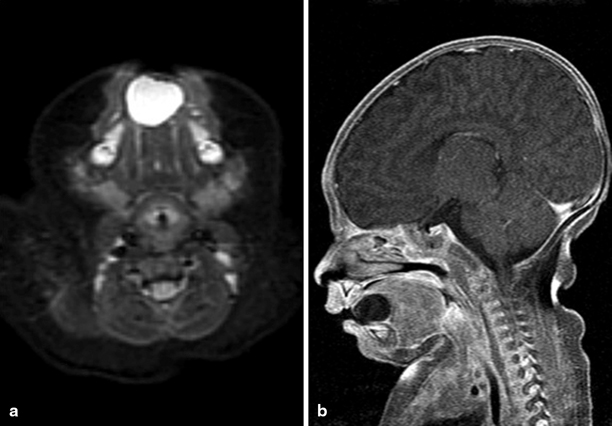
Fig. 19.2
A 7-week-old girl with a tongue foregut duplication cyst. a An axial fast spin-echo inversion recovery MRI reveals a unilocular, sharply circumscribed midline lesion that is isointense with cerebrospinal fluid located within the anterior aspect of the floor of the mouth. b A gadolinium-enhanced, fat-suppressed sagittal T1-weighted image reveals a cystic mass that does not enhance
Studies have noted the association of vertebral anomalies with foregut duplication cysts, termed neurenteric cysts, since the cyst interferes with anterior fusion of the vertebral mesoderm . However, in the largest reported series of head and neck foregut duplication cysts, no patient had any vertebral or spinal anomalies noted on CT or MRI.
With the increased use of maternal ultrasound, cystic lesions are being diagnosed antenatally. Foregut duplication cysts have been identified in this manner and may potentially warrant emergent airway management at birth including consideration of a potential EXIT procedure [7].
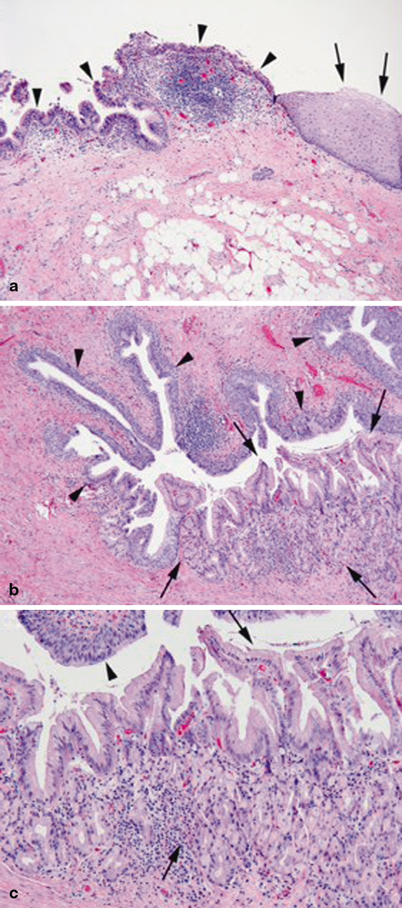
Pathology
Traditionally, there are three pathological criteria (Fig. 19.3) that must be met in order to make a diagnosis of foregut duplication cyst [8]: