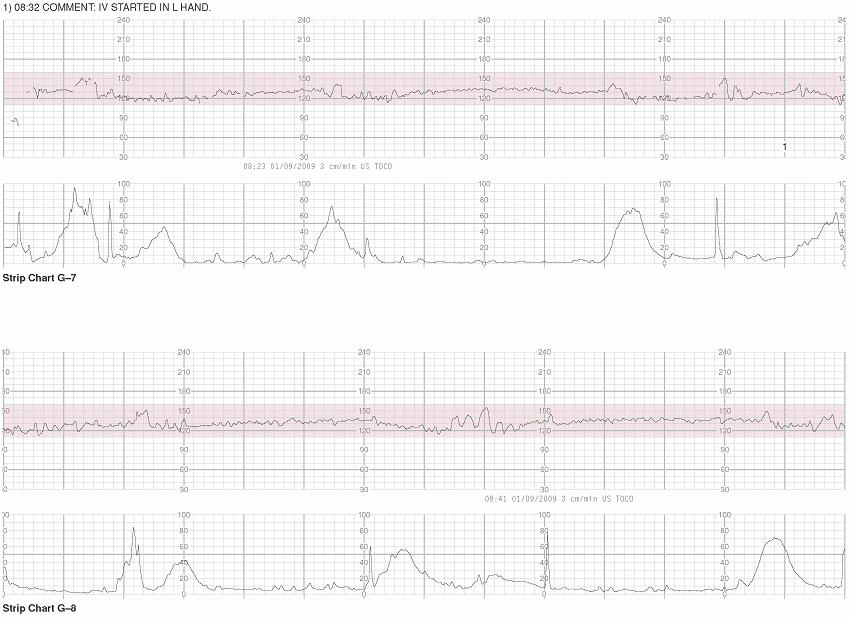
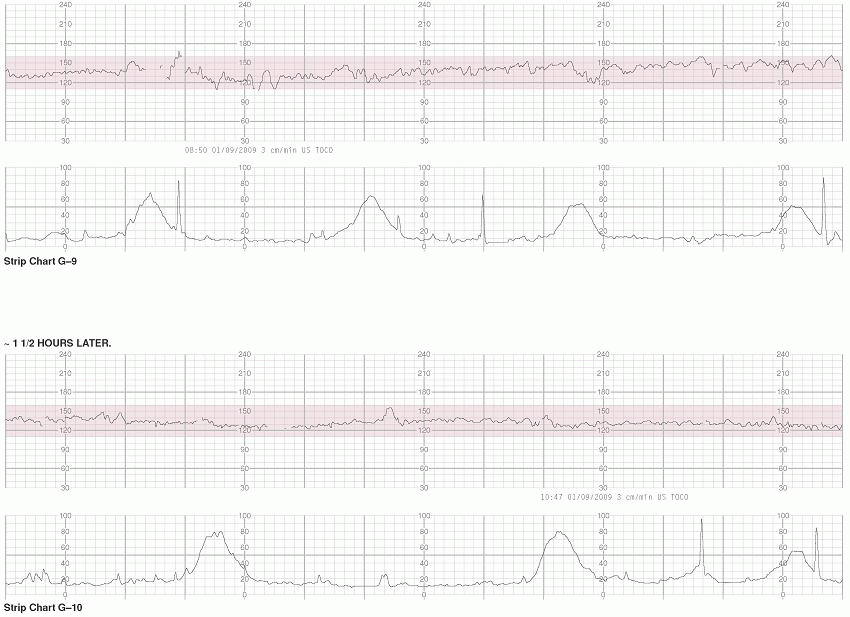
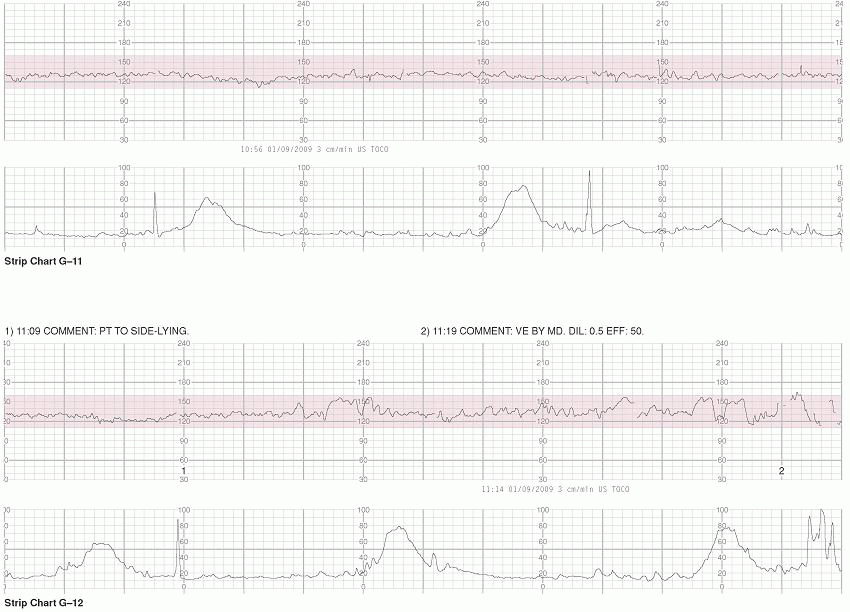
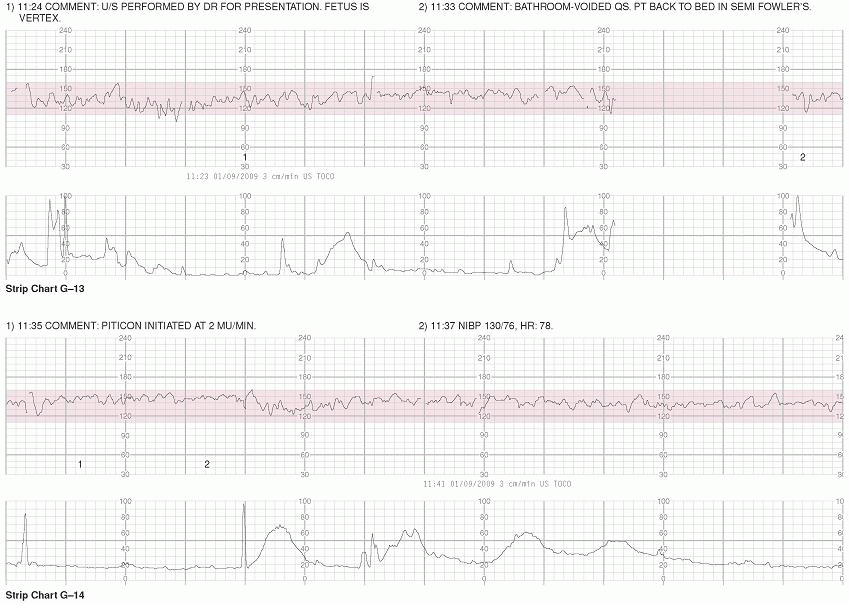
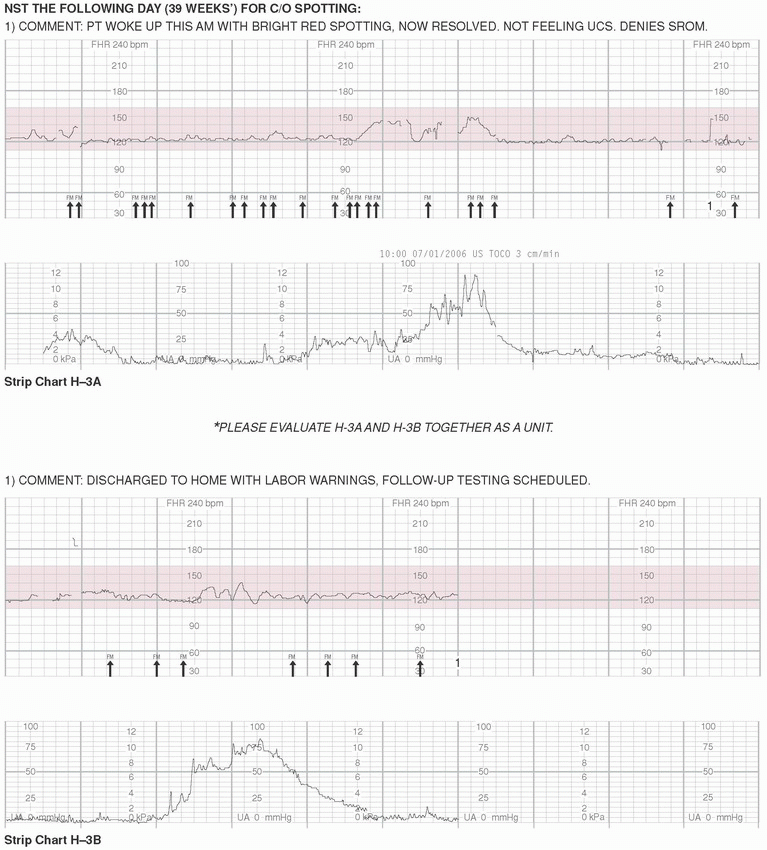
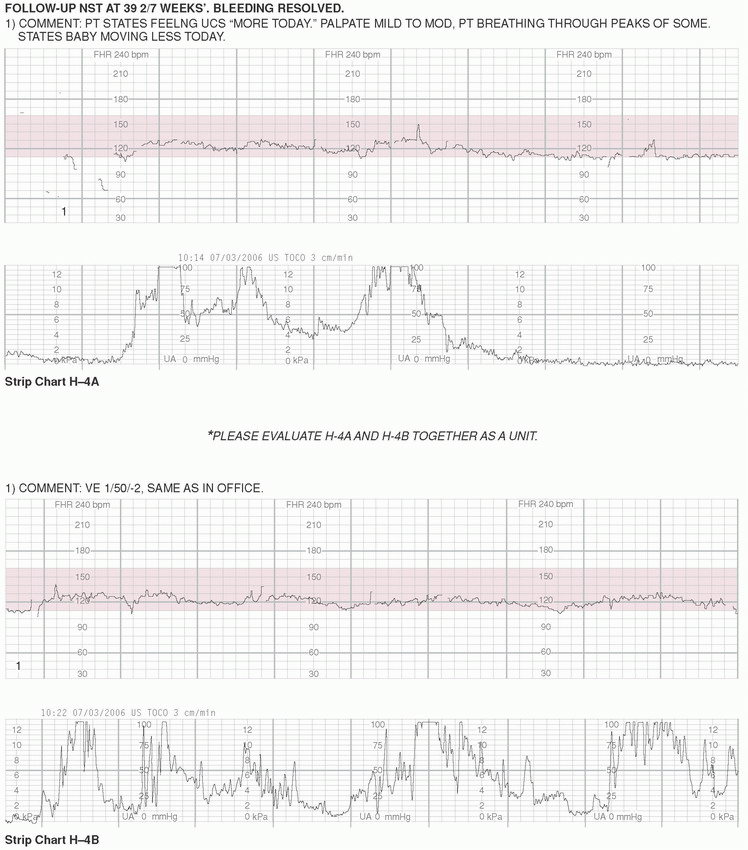
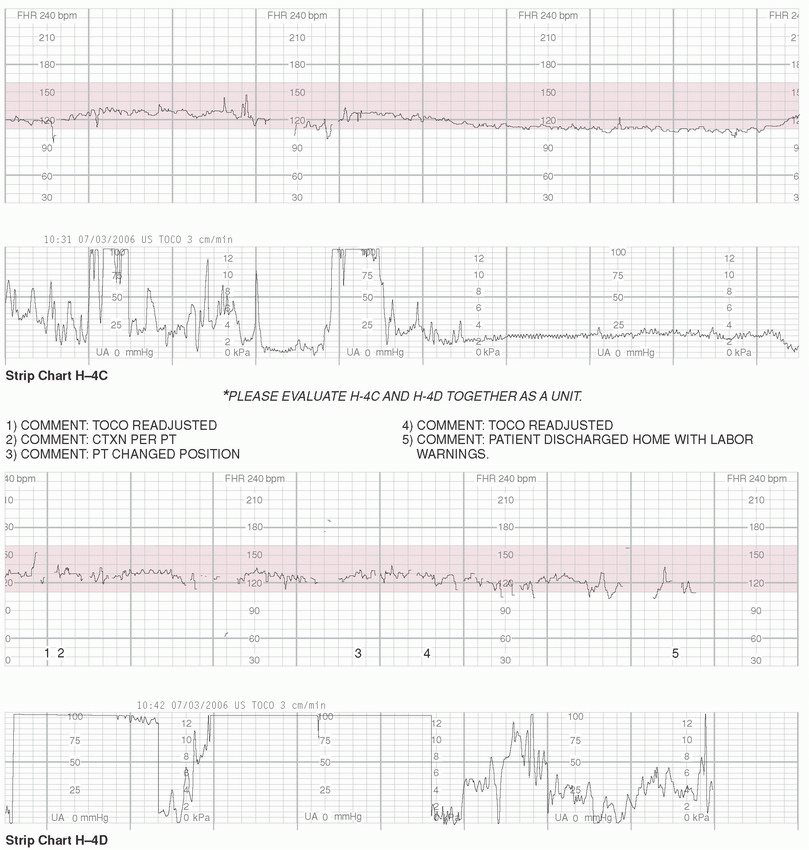
The exercises presented in this chapter are meant to facilitate the integration of the didactic information contained within the text of this book into the processes of critical thinking necessary for practicing the skill of electronic fetal monitoring (EFM). In each of the following case studies, select portions of the fetal strip chart are presented along with the contemporaneous nurse’s notes. When gaps in the data occur, the passage of time is denoted at the start of the subsequent portion of the fetal strip chart.
Proper completion of the exercises includes comparison of one’s interpretation of the fetal strip with the Guide to Interpretation that is located at the end of this chapter. It is necessary to recognize that the information presented within the case studies has been preserved for the purpose of being as accurately reflective of actual circumstances as is possible without breaching confidentiality. Therefore, the interpretations and interventions presented within each case study are not necessarily reflective of the best practices or current standard of care. Comparison with the Guide to Interpretation (located in the second half of this chapter) and with current, evidence-based practice is essential in promoting appropriate clinical decision making. The Guide to Interpretation is based upon the reasoning and parameters for evaluating EFM data as have been explained throughout the preceding chapters. Minor variations in interpretation are expected to occur as a result of multiple factors (as discussed in Chapters 3 and 7); that is, there may be some insignificant differences between readers’ interpretations or between the reader and authors’ interpretations.
For purposes of confidentiality, all proper pronouns have been removed from the case studies. All other identifying data have been altered to protect the privacy of the patient. Only the clinical designation of the person mentioned (e.g., RN, CNM, MD, etc.) is presented.
The commentary appearing above the strip chart corresponds with the numerical annotations located in the center margin of the paper strip chart. Abbreviations and nomenclature may vary from case to case, based on regional or individual differences in expression (e.g., use of the terms UC or CTX to express uterine contraction).
For the purposes of clarity and consistency, the Guide to Interpretation at the end of this chapter utilizes the terminology suggested by the 2008 National Institute of Child Health and Human Development Workshop Report on Electronic Fetal Monitoring (see Chapter 3).1 When the case studies present monitoring of uterine activity (UA) through use of an intrauterine pressure catheter (IUPC), the strength of contractions is expressed in a peak-minus-baseline format. It is necessary to recognize that the selected methods for expressing interpretation of the strip chart employed in the Guide to Interpretation may not be reflective of individual institutional standards or culture. Additionally, minor interobserver variations in interpretation are likely to occur. Such differences should be viewed objectively and utilized as a catalyst for discussion and continued learning.
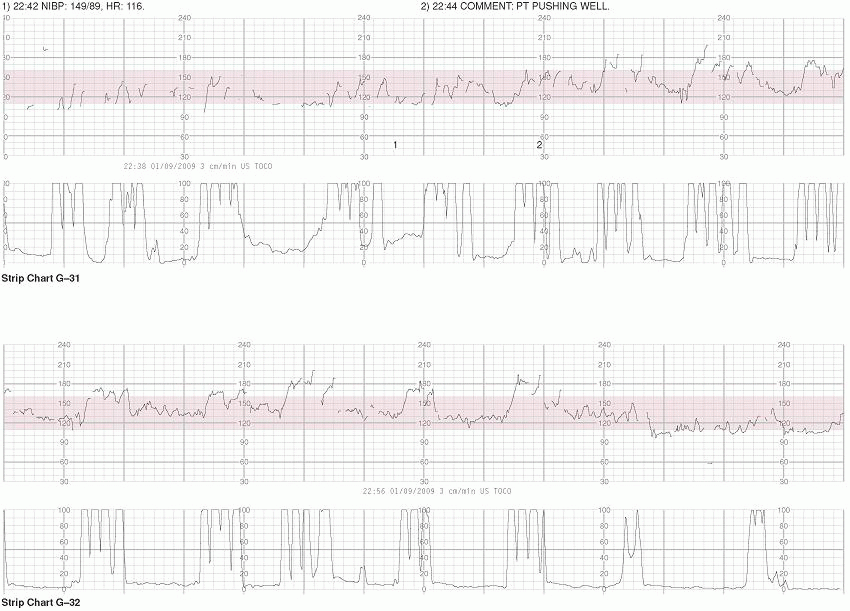
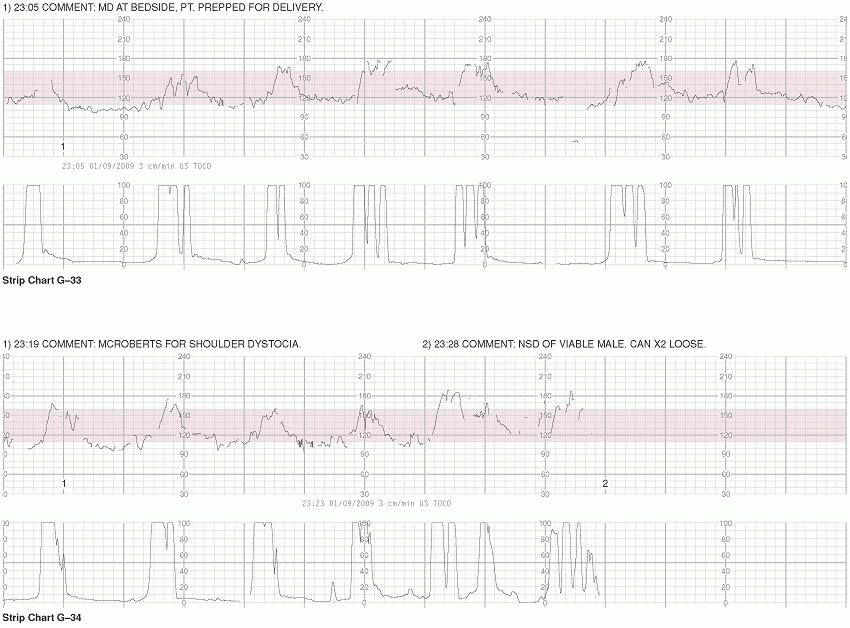
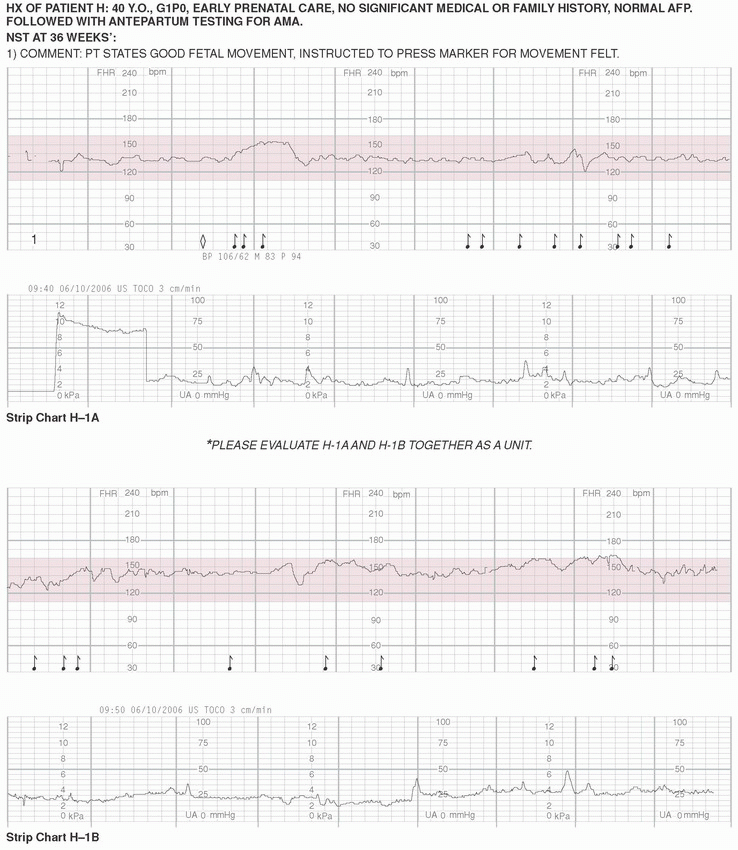
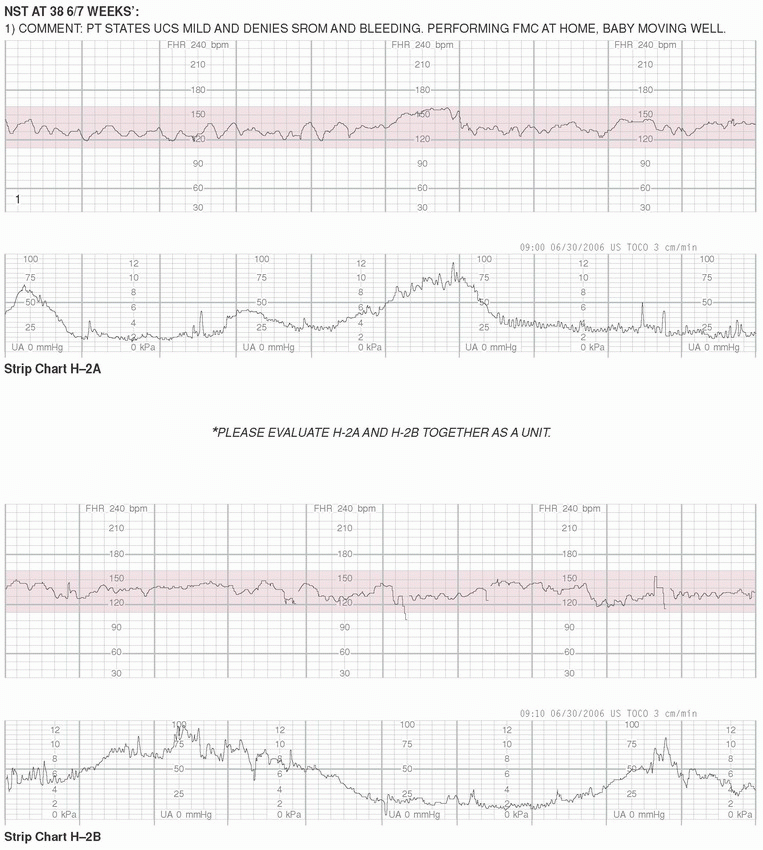
The case studies are presented on strip charts that are printed with 30-240 bpm paper scaling. Because the examples are presented at 3 cm/min paper speed, each regularly occurring vertical marker represents the passage of 10 seconds of time. Every sixth vertical line is emphasized to represent the passage of 1 minute of time (six 10-second segments).
It is necessary assess both the mother and fetus at regular intervals as dictated by institutional policy. These assessments should be documented, and any necessary interventions performed should be communicated to the care provider and to any other personnel who may need to know, such as the charge nurse. Regular assessment of the fetus includes systematic evaluation of the fetal heart rate (FHR) as described in Chapter 3. Common, standardized, and descriptive terminology should be used by care providers and registered nurses to communicate information about the FHR.2 Such assessments are ordinarily performed at least every 30 minutes during the active phase of the first stage of labor and at least every 15 minutes during the second stage. In the presence of risk factors, or with use of oxytocin, the FHR is usually evaluated at least every 15 minutes during the active phase of the first stage of labor and at least every 5 minutes during the second stage.2, 3 and 4 It is important to be aware of institutional policies on evaluation and documentation and also utilize clinical judgment to respond appropriately to individual clinical circumstances. The exercises in this chapter (Box 5-1) provide the opportunity to practice systematic assessment of the FHR. These FHR strips are available on http://solution.lww.com and additional exercises will be added to this website periodically.
BOX 5-1 Case Review Worksheet for Chapter 5 Exercises
Photocopy the blank worksheet for convenience in practicing charting on segments of the example tracings.
STRIP CHART #
Fetal Heart Rate
Uterine Activity
Baseline:
Frequency:
Variability:
Duration:
Periodic/Episodic Changes:
Strength:
Resting Tone:
Category (circle one):
I
II
III
STRIP CHART #
Fetal Heart Rate
Uterine Activity
Baseline:
Frequency:
Variability:
Duration:
Periodic/Episodic Changes:
Strength:
Resting Tone:
Category (circle one):
I
II
III
STRIP CHART #
Fetal Heart Rate
Uterine Activity
Baseline:
Frequency:
Variability:
Duration:
Periodic/Episodic Changes:
Strength:
Resting Tone:
Category (circle one):
I
II
III
STRIP CHART #
Fetal Heart Rate
Uterine Activity
Baseline:
Frequency:
Variability:
Duration:
Periodic/Episodic Changes:
Strength:
Resting Tone:
Category (circle one):
I
II
III
Case Examples
Guide to Interpretation
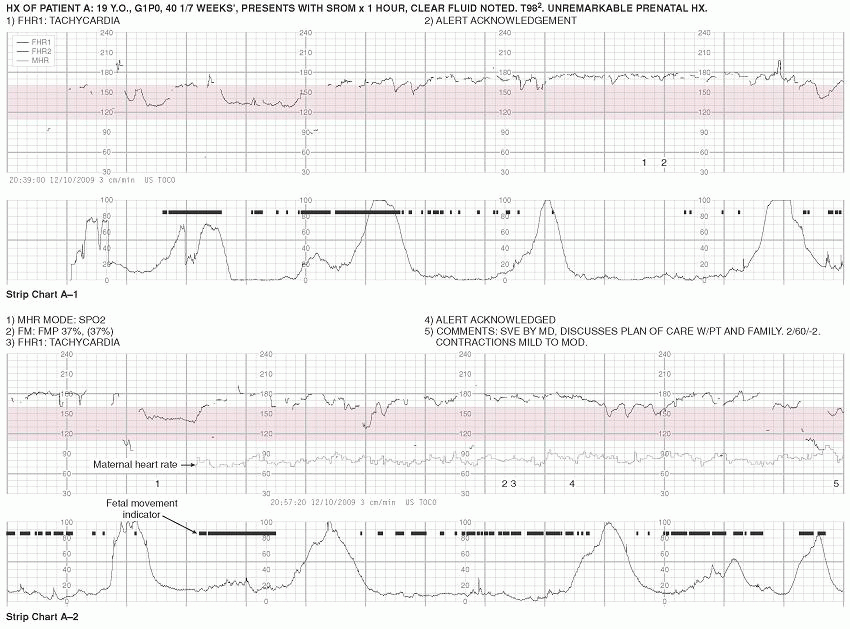
STRIP CHART A-1
Fetal Heart Rate
Uterine Activity
Baseline:
175 bpm
Frequency:
1-4 minutes
Variability:
Moderate
Duration:
1-2 minutes
Periodic/Episodic Changes:
Variable Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: Patient presents with what appears to be a fetal tachycardia. She is not febrile; however, her temperature should be monitored closely in light of this finding. A careful history should be taken, including inquiry about possible drug (OTC or illicit) or herbal use, and consideration to activity level, weather/environment, and nutritional status/hydration prior to admission. IV hydration should be considered promptly.
STRIP CHART A-2
Fetal Heart Rate
Uterine Activity
Baseline:
175 bpm
Frequency:
2-4.5 minutes
Variability:
Moderate
Duration:
60-90 seconds
Periodic/Episodic Changes:
Variable and Late Decelerations
Strength:
Mild-Moderate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: Maternal heart rate and fetal movement are additional parameters that are being recorded on the tracing. It is noteworthy that the portion of the FHR that presently is considered baseline (and demonstrates fetal tachycardia) appears to coincide with fetal movement. It would be helpful to the assessment to have the bedside impression of what is occurring; for example, whether the fetus is heard on the monitor, observed through the abdomen, or noted by the mother to be experiencing a period of excessive movement.
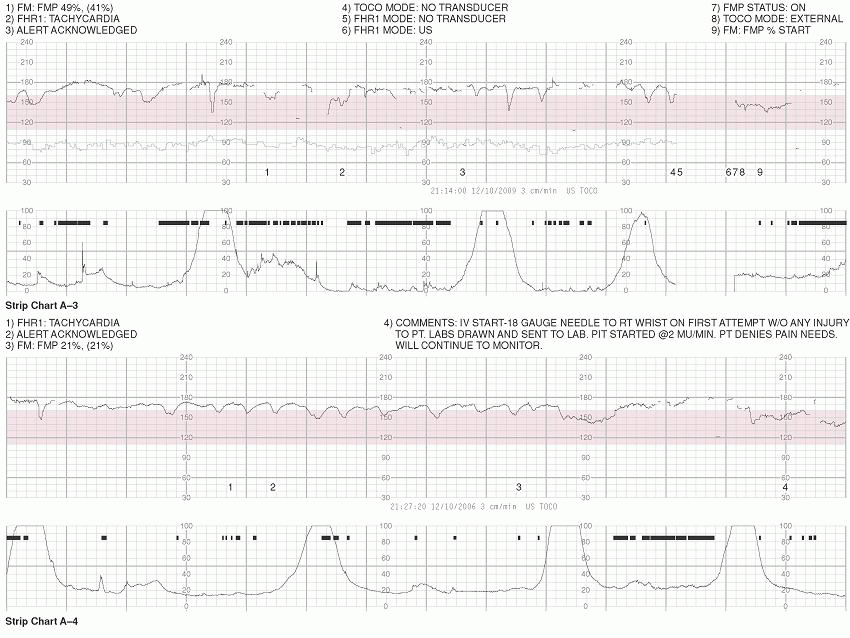
STRIP CHART A-3
Fetal Heart Rate
Uterine Activity
Baseline:
170 bpm
Frequency:
2.5-5 minutes
Variability:
Moderate
Duration:
1-3 minutes
Periodic/Episodic Changes:
Variable Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
STRIP CHART A-4
Fetal Heart Rate
Uterine Activity
Baseline:
165 bpm
Frequency:
3-5 minutes
Variability:
Moderate
Duration:
1-2 minutes
Periodic/Episodic Changes:
Variable Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: The FHR has taken on a somewhat odd appearance that bears observation. It may be advisable to delay starting oxytocin until this pattern is resolved. Internal FHR monitoring (FECG) with a spiral electrode may also be considered for closer observation.
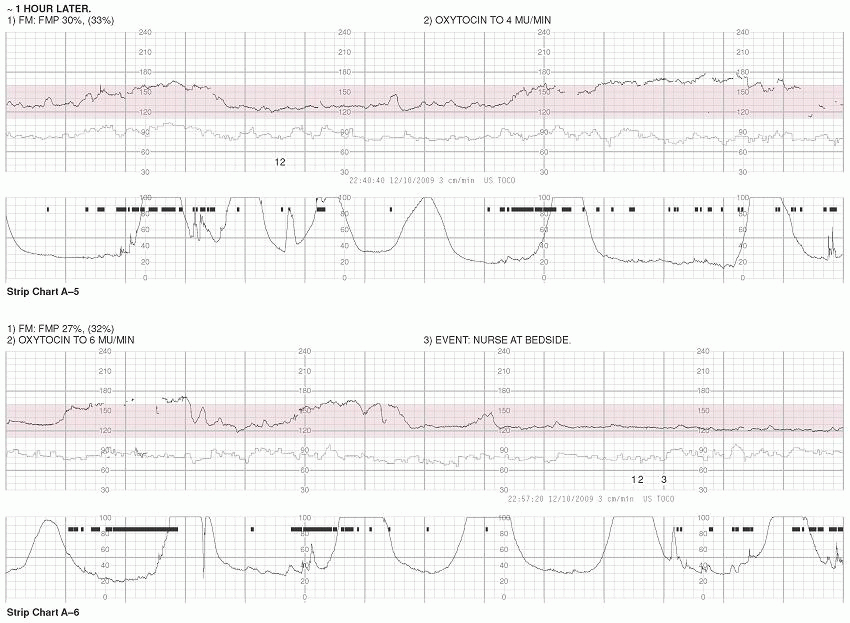
STRIP CHART A-5
Fetal Heart Rate
Uterine Activity
Baseline:
165 bpm
Frequency:
1-4 minutes
Variability:
Moderate
Duration:
70-90 seconds
Periodic/Episodic Changes:
Prolonged Deceleration
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: During the optimal portion of this tracing to observe the FHR (the area between the last two contractions), the FHR baseline appears to be 165 bpm. It is logical that during the period of hypercontractility (starting 2 minutes into the tracing and continuing for 6 minutes), the FHR would decelerate. However, once again, it appears that the episodes of tachycardia coincide with period of fetal movement and commentary of bedside observation may provide further clarification.
STRIP CHART A-6
Fetal Heart Rate
Uterine Activity
Baseline:
125 bpm
Frequency:
2-2.5 minutes
Variability:
Minimal-Moderate
Duration:
2 minutes
Periodic/Episodic Changes:
Accelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
Discussion: Approximately 2 hours after admission, the FHR is beginning to look quite different. It is always important to compare for changes over time. The baseline is no longer seems to be tachycardic and episodes of fetal movement coincide with what now appear to be accelerations of the FHR. The contraction pattern bears consideration, as contractions are occurring frequently and are lengthy and there does not appear to be adequate (at least 1 minute) uterine rest between them. More information regarding bedside clinical observation would be helpful, including findings of palpation of abdomen during and in between contractions.
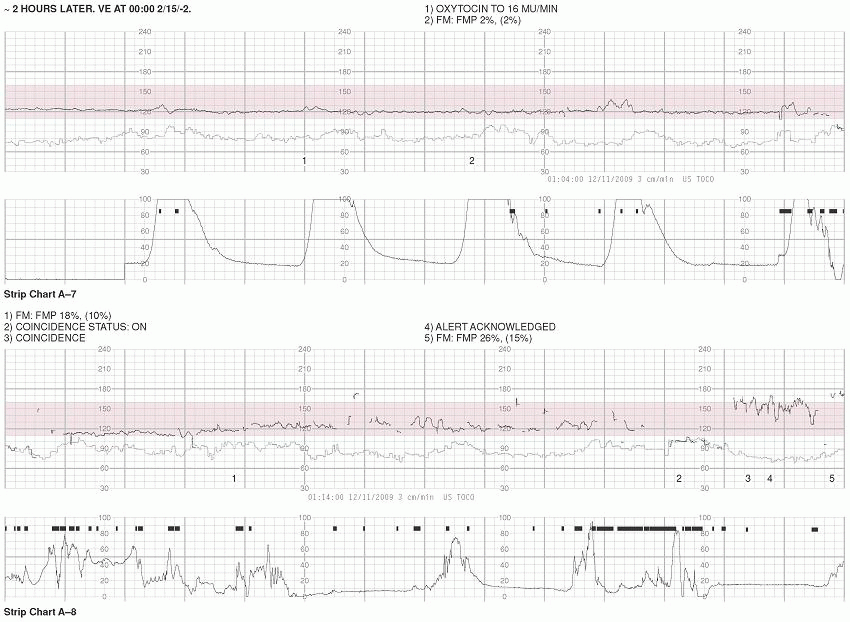
STRIP CHART A-7
Fetal Heart Rate
Uterine Activity
Baseline:
120 bpm
Frequency:
2-3 minutes
Variability:
Minimal-Moderate
Duration:
60-90 seconds
Periodic/Episodic Changes:
Acceleration
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
STRIP CHART A-8
Fetal Heart Rate
Uterine Activity
Baseline:
125 bpm
Frequency:
1-3.5 minutes
Variability:
Moderate
Duration:
40 seconds-2 minutes (?)
Periodic/Episodic Changes:
Acceleration
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
Discussion: During the last 2 minutes of the tracing, the FHR recording takes on an odd appearance (increased variability and higher rate) at the same time that a “coincidence” alert occurs. Some monitors can have the ability to differentiate between two heart rates (FHR and MHR, or between the FHR patterns of twins). This is helpful when both rates are similar. It is likely that this patch of recording reflects a brief period of double counting the MHR, rather than an actual representation of the FHR. It is essential to be familiar with the capabilities and features of the equipment used in your setting in order to fully understand the data presented. UA is difficult to assess as tocotransducer needs adjustment.
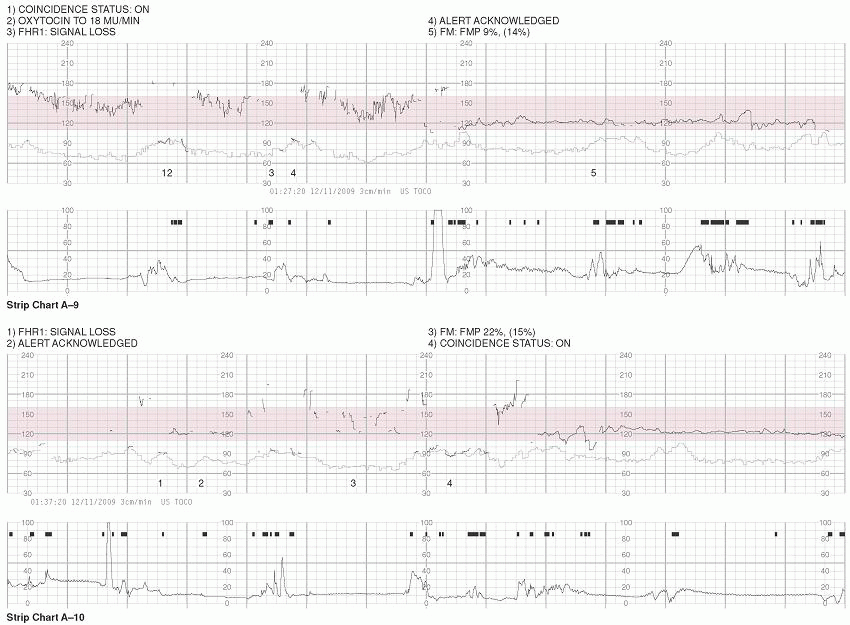
STRIP CHART A-9
Fetal Heart Rate
Uterine Activity
Baseline:
120 bpm
Frequency:
Tocotransducer not recording adequately
Variability:
Moderate
Duration:
Tocotransducer not recording adequately
Periodic/Episodic Changes:
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
Discussion: It appears that the MHR continues to be erroneously obtained by the ultrasound transducer, producing a recording of double-counting of the MHR during the first half of this tracing. Once the monitor is adjusted, the FHR recording returns. It is necessary that closer attention be paid to monitoring of UA.
STRIP CHART A-10
Fetal Heart Rate
Uterine Activity
Baseline:
120 bpm
Frequency:
Tocotransducer not recording adequately
Variability:
Minimal-Moderate
Duration:
Tocotransducer not recording adequately
Periodic/Episodic Changes:
Indeterminate
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
Discussion: In the first half of this tracing, there continues to be a loss of FHR signal acquisition and contractions continue to not be recording. With oxytocin infusing, it is essential to have continuous information about both the FHR and UA. The external monitors need to be adjusted or internal monitoring considered.
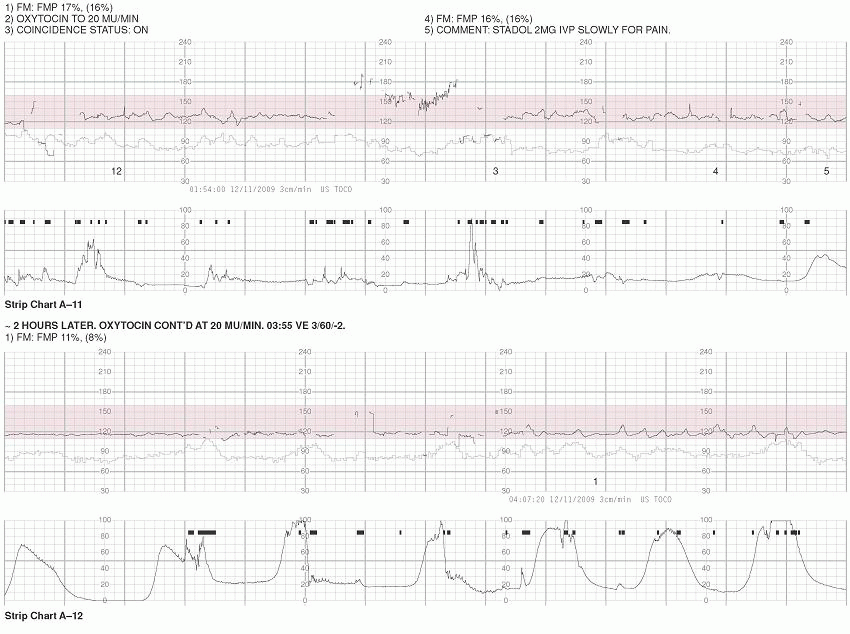
STRIP CHART A-11
Fetal Heart Rate
Uterine Activity
Baseline:
125 bpm
Frequency:
Tocotransducer not recording adequately
Variability:
Moderate
Duration:
Tocotransducer not recording adequately
Periodic/Episodic Changes:
None
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
STRIP CHART A-12
Fetal Heart Rate
Uterine Activity
Baseline:
120 bpm
Frequency:
1.5-2 minutes
Variability:
Moderate
Duration:
1-2 minutes
Periodic/Episodic Changes:
None
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
Discussion: In approximately 7 hours and with 20 mU/min of oxytocin infusing, the patient has progressed 1 cm. Any effects on the FHR from the Stadol (decreased variability) given 2 hours prior should be resolved by this time.
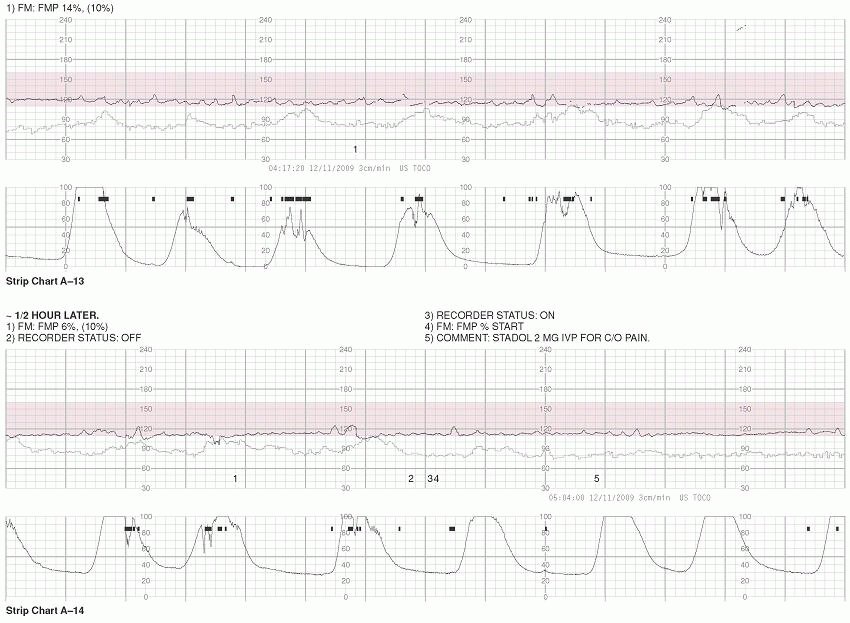
STRIP CHART A-13
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
1.5-2.5 minutes
Variability:
Moderate
Duration:
60-80 seconds
Periodic/Episodic Changes:
None
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
STRIP CHART A-14
Fetal Heart Rate
Uterine Activity
Baseline:
110 bpm
Frequency:
1-2.5 minutes
Variability:
Minimal-Moderate
Duration:
60-90 seconds
Periodic/Episodic Changes:
None
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
Discussion: Although the contraction pattern does not technically qualify as tachysystole (>5 contractions/10 min), it is on the borderline and warrants observation. Internal monitoring (IUPC) could be helpful.
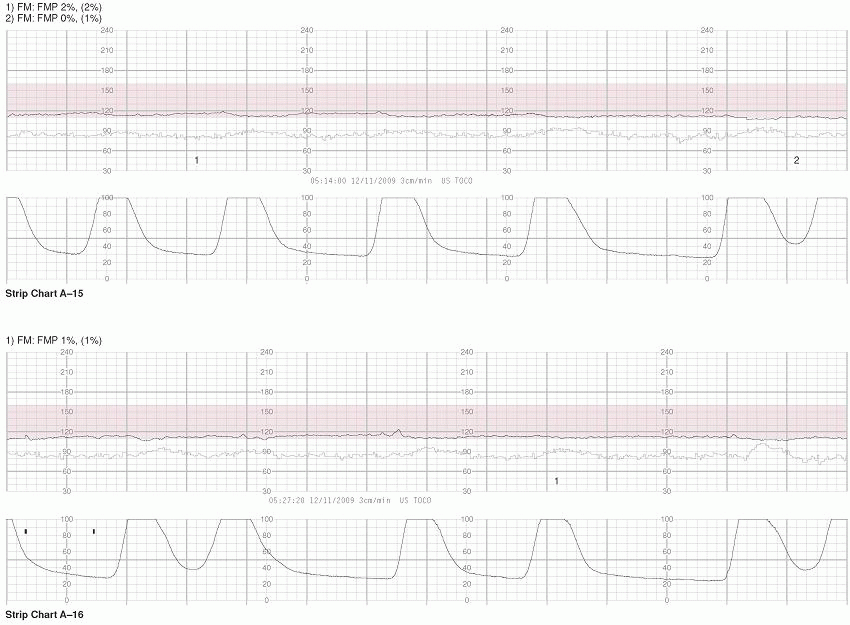
STRIP CHART A-15
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
1-2.5 minutes
Variability:
Minimal
Duration:
60-90 seconds
Periodic/Episodic Changes:
Early Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
STRIP CHART A-16
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
1-3 minutes
Variability:
Minimal
Duration:
80 seconds-2 minutes
Periodic/Episodic Changes:
Early Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
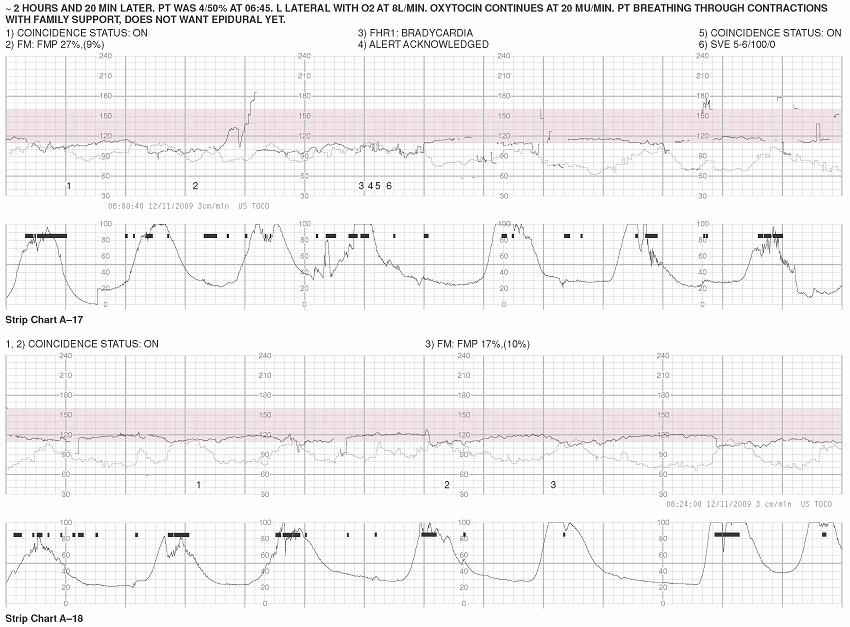
STRIP CHART A-17
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
1.5-3 minutes
Variability:
Minimal
Duration:
80 seconds-2 minutes
Periodic/Episodic Changes:
Early and Late Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
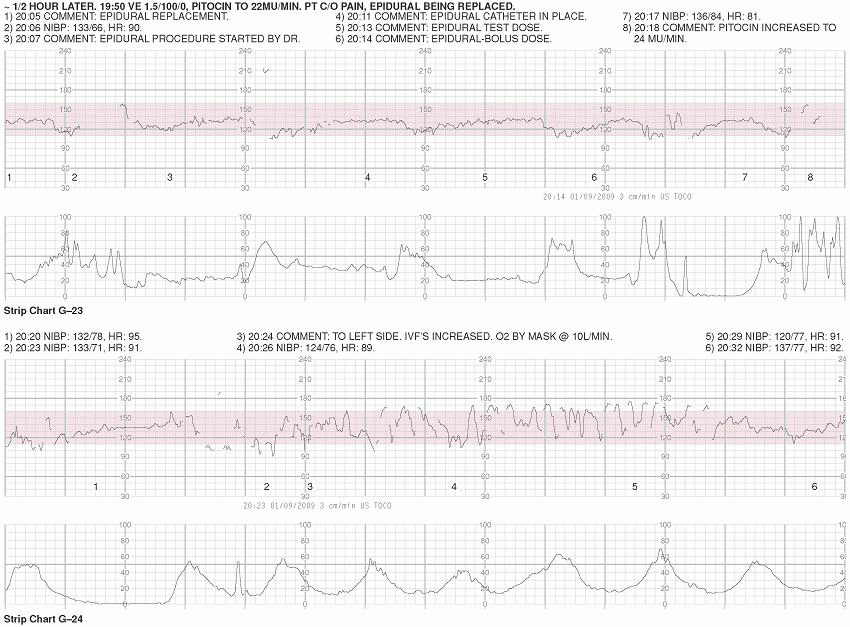
Discussion: In 3 hours, the patient has progressed 1 cm. Since the most recent exam 1.5 hours prior, she progressed 1.5 cm and went from 50% to 100% effacement. The UC pattern continues to push the limits of normal in terms of frequency and duration of contractions and should be evaluated. By now, the effects of the second dose of Stadol on the fetus should be resolved. The actions to implement intrauterine resuscitation are prudent; however, this would warrant greatly decreasing or discontinuing the oxytocin and include administration of oxygen at 10 L/min (via nonrebreather mask), increasing IV fluids (1,000-cc bolus), and having the tracing evaluated by the care provider.
STRIP CHART A-18
Fetal Heart Rate
Uterine Activity
Baseline:
120 bpm
Frequency:
2-2.5 minutes
Variability:
Minimal
Duration:
90-140 seconds
Periodic/Episodic Changes:
Early Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
STRIP CHART A-19
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
60-80 seconds
Variability:
Minimal
Duration:
80 seconds-3 minutes
Periodic/Episodic Changes:
Early Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: The UC pattern is tachysystole and should be addressed by turning down or turning off the oxytocin and consulting with the care provider.
STRIP CHART A-20
Fetal Heart Rate
Uterine Activity
Baseline:
120 bpm
Frequency:
1-3 minutes
Variability:
Minimal-Moderate
Duration:
1-2 minutes
Periodic/Episodic Changes:
Early and Late Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
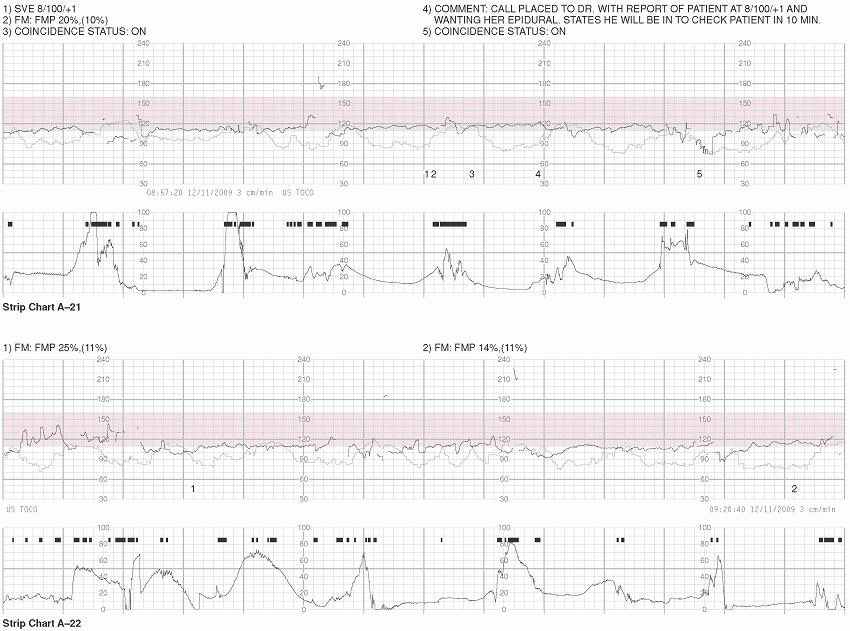
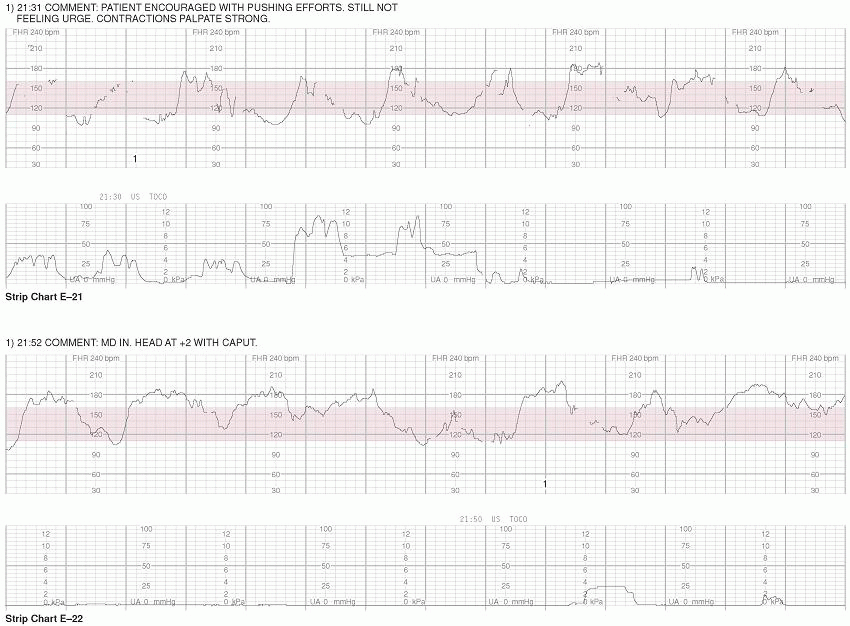
STRIP CHART A-21
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
1-2.5 minutes
Variability:
Moderate
Duration:
1-2 minutes
Periodic/Episodic Changes:
Early and Variable Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
STRIP CHART A-22
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
1-3 minutes
Variability:
Minimal-Moderate
Duration:
50 seconds-2 minutes
Periodic/Episodic Changes:
Early Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
I
II
III
Discussion: It is difficult to categorize the deceleration pattern (early vs. late) when the UCs are not clearly recorded.
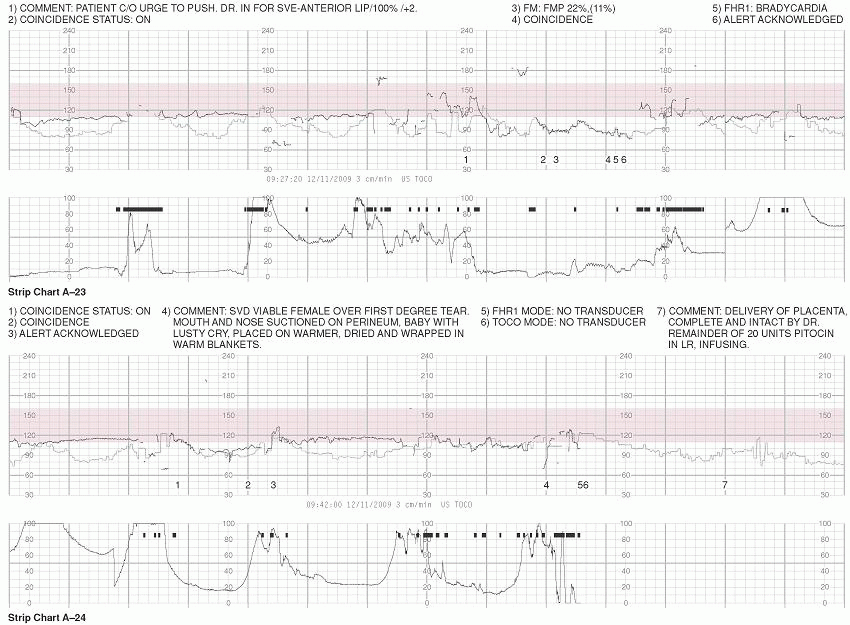
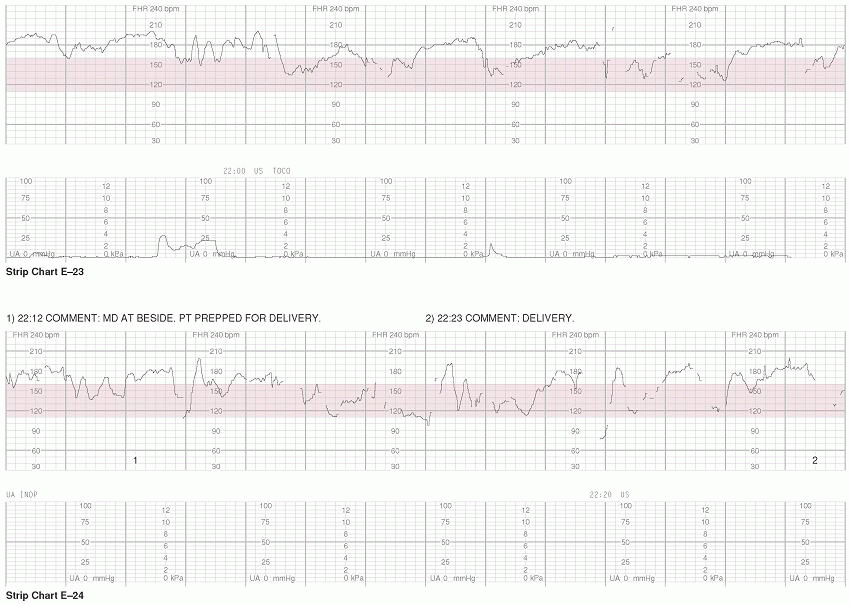
STRIP CHART A-23
Fetal Heart Rate
Uterine Activity
Baseline:
110 bpm
Frequency:
Indeterminate
Variability:
Minimal
Duration:
Indeterminate
Periodic/Episodic Changes:
Prolonged Deceleration
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
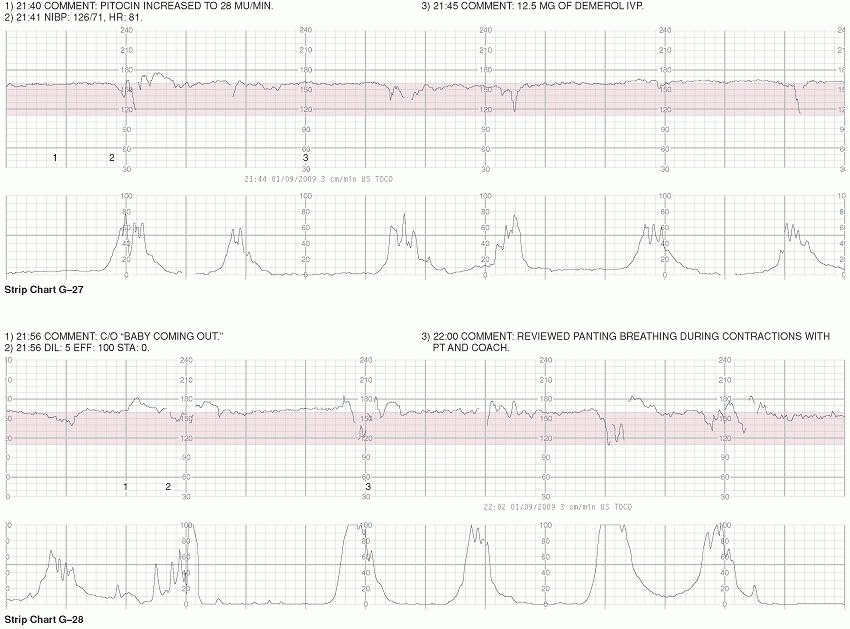
Discussion: At this time, with the patient near fully dilated and feeling the urge to push and the tracing with minimal variability and decelerations, decreasing or discontinuing the oxytocin should be considered. The patient is a primip, and the length of her pushing (which puts further stress on the fetus) is unknown. Physiologic pushing (open glottis, pushing with the urge) and pushing on her side could be useful techniques in this instance.
STRIP CHART A-24
Fetal Heart Rate
Uterine Activity
Baseline:
115 bpm
Frequency:
2-2.5 minutes
Variability:
Minimal
Duration:
90 seconds
Periodic/Episodic Changes:
Late and Prolonged Deceleration
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
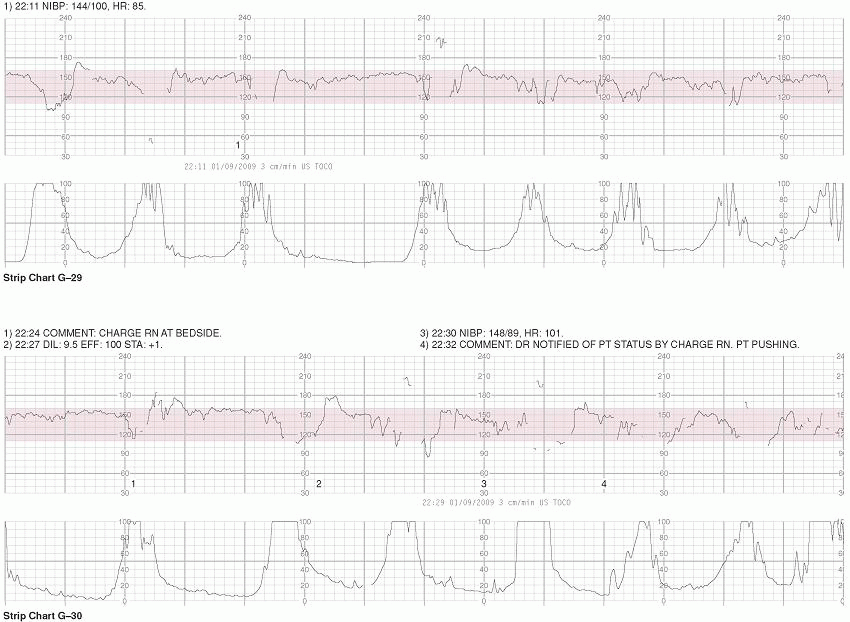
Discussion: Fortunately, the pushing phase was relatively short (<30 minutes), minimizing the amount of stress on the fetus.
OUTCOME: Female delivered at 09:46. Apgars 9/10, weight 3,062 g (6 lb, 12 oz). Short cord – 28 cm (11 inches) noted.
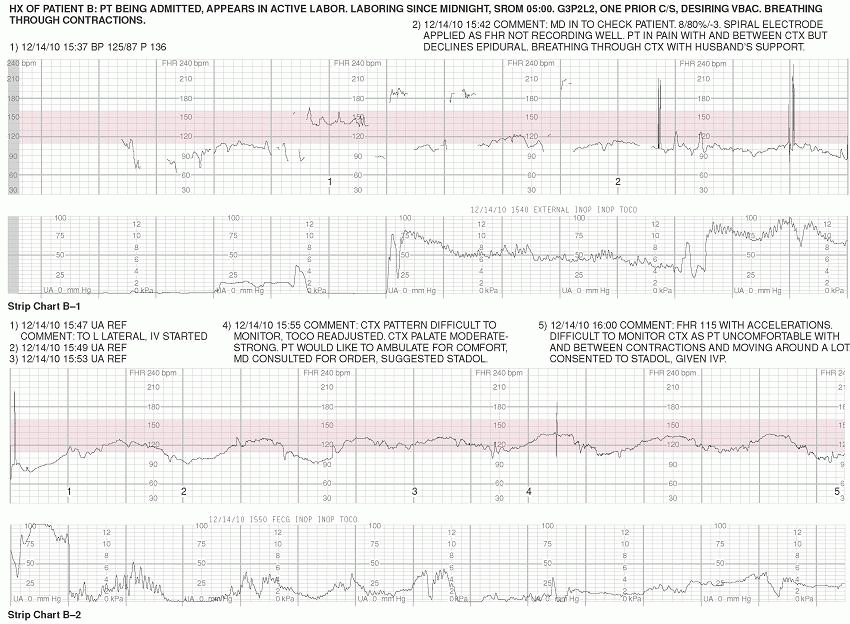
STRIP CHART B-1
Fetal Heart Rate
Uterine Activity
Baseline:
105 bpm
Frequency:
Indeterminate
Variability:
Moderate
Duration:
Indeterminate
Periodic/Episodic Changes:
Variable Decelerations (?)
Strength:
Indeterminate
Resting Tone:
Indeterminate
Category:
II
Discussion: It is challenging to interpret this portion of tracing. The data that is available, however, warrants close observation, as it does not fall within normal parameters (110-160 bpm). The brief excursions of an FHR >180 could indicate double-counting of a very fetal low heart rate, an issue that can usually be ruled out with use of internal FHR monitoring (FECG), as this mode of monitoring has a greater range (see Chapter 2). With a lower than normal heart rate, information about the maternal pulse is essential. If there is any doubt about which signal (maternal or fetal) is being recorded, it is important to palpate for maternal pulse and simultaneously compare findings with the audible signal from the electronic fetal monitor. Concerns about UA in this segment of tracing include the patient experiencing pain not only with, but also between, contractions and the inability to record contraction data.
STRIP CHART B-2
Fetal Heart Rate
Uterine Activity
Baseline:
130 bpm
Frequency:
Indeterminate
Variability:
Minimal
Duration:
Indeterminate
Periodic/Episodic Changes:
Late decelerations (?)
Strength:
Indeterminate
Resting Tone:
Indeterminate
Category:
II
Discussion: The FHR baseline is difficult to ascertain, primarily as there is no clear UA data against which to evaluate. It is unlikely, however, that the FHR is 115 bpm with accelerations as noted. It would make sense, however, for the maternal heart rate (MHR) to be elevated during contractions in response to increased pain. At this time, it is essential to clarify the UA pattern (monitor internally with an IUPC if an external tracing cannot be maintained). It is concerning that the patient is in pain not only with, but also between contractions, particularly because she is a VBAC (placing her at risk for uterine rupture). Continuous pain is a common symptom of uterine rupture. As the tracing is suspect and the patient’s condition not verified, allowing the patient to ambulate would not be advisable at this time.
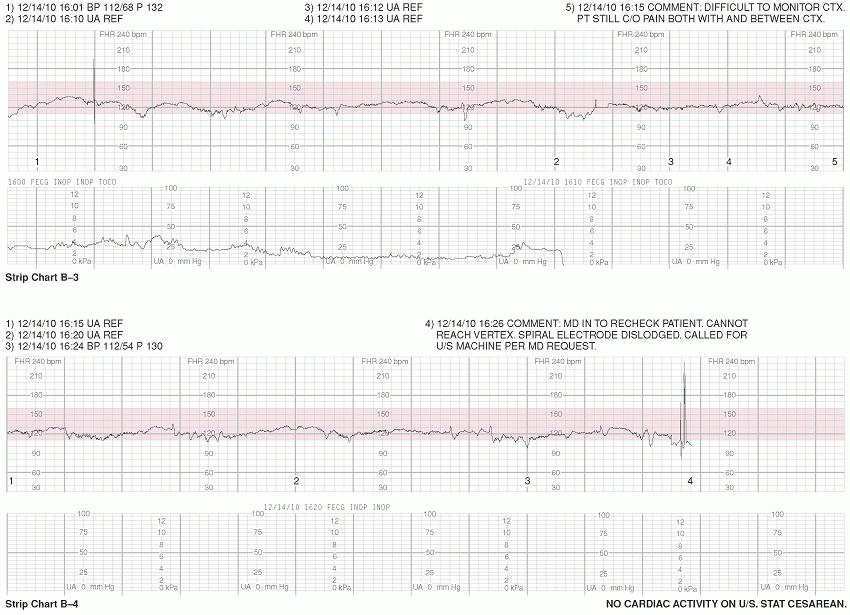
STRIP CHART B-3
Fetal Heart Rate
Uterine Activity
Baseline:
125 bpm
Frequency:
Indeterminate
Variability:
Minimal
Duration:
Indeterminate
Periodic/Episodic Changes:
Late decelerations (?)
Strength:
Indeterminate
Resting Tone:
Indeterminate
Category:
II
Discussion: Concerns regarding the maternal and fetal condition continue as noted above. Maternal vital signs should be considered within the context of the clinical picture. Although it appears that the tocotransducer has been adjusted numerous times, this essential data continues to not be recorded. With pain medicine now in effect, the “accelerations” (as they are described in the charting) in the heart rate during contractions are no longer present, another piece of evidence consistent with a MHR pattern (the patient is not in as much pain during contractions; therefore, her heart rate is no longer markedly increasing in response).
STRIP CHART B-4
Fetal Heart Rate
Uterine Activity
Baseline:
125 bpm
Frequency:
Indeterminate
Variability:
Minimal
Duration:
Indeterminate
Periodic/Episodic Changes:
Late decelerations (?)
Strength:
Indeterminate
Resting Tone:
Indeterminate
Category:
II
Discussion: Concerns regarding the maternal and fetal condition continue as noted above.
OUTCOME: The fetus is delivered via Cesarean at 16:46 with Apgars of 0/0, diagnosis of uterine rupture confirmed. Resuscitation: A full neonatal code ensued but was not successful. The entire recording was of the MHR. At no time was an FHR acquired or represented on the tracing. Please see Chapter 2 for detailed information about erroneous recording of MHR.
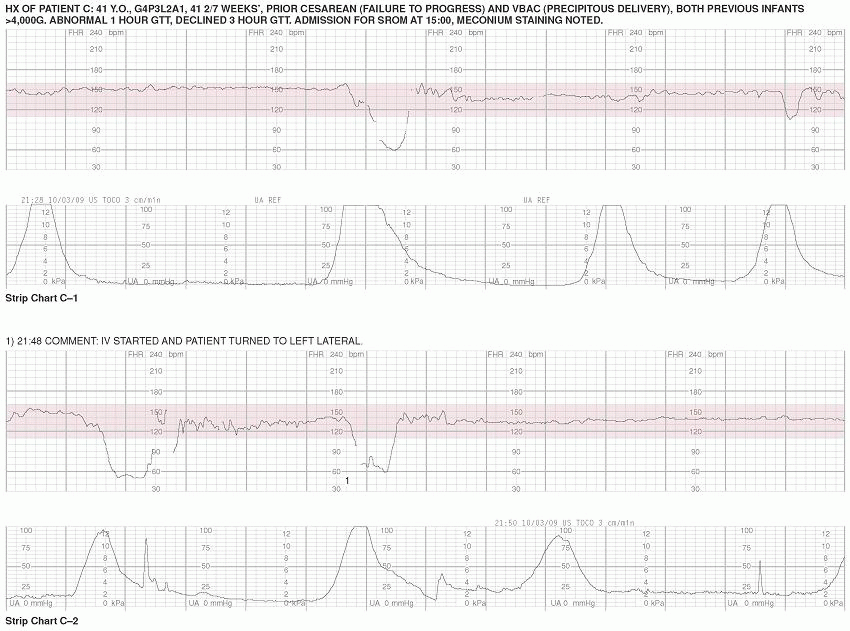
STRIP CHART C-1
Fetal Heart Rate
Uterine Activity
Baseline:
150 bpm
Frequency:
3-5 minutes
Variability:
Moderate
Duration:
90 seconds-3 minutes
Periodic/Episodic Changes:
Intermittent Late and Variable Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: It is important to keep in mind throughout review of this tracing (and certainly as the providers assessing it in real time) that his patient presents as high risk; she is of advanced maternal age, postdates, and attempting VBAC. Additionally, her two children were macrosomic at birth and she had an abnormal 1-hour GTT with this pregnancy, indicators that this fetus also may be large. Many of the decelerations in this case do not precisely demonstrate the characteristics of any one specific type of deceleration per NICHD definitions but, rather, overlaps two classifications (variable decelerations and late decelerations). Therefore, discrepancies in interpretation may occur. Regardless of whether these decelerations are deemed to be variable or late, both types represent diminished oxygenated blood flow to the fetus and should be treated as such. Ultimately, it is a provision of appropriate clinical response that is of paramount importance.
STRIP CHART C-2
Fetal Heart Rate
Uterine Activity
Baseline:
140 bpm
Frequency:
3-5 minutes
Variability:
Minimal
Duration:
2 minutes
Periodic/Episodic Changes:
Late Decelerations
Strength:
Tocotransducer in place—must palpate
Resting Tone:
Tocotransducer in place—must palpate
Category:
II
Discussion: In most other aspects, these decelerations match of the definition of the visual appearance of a variable deceleration; however, they do not reach their nadir in ≥30 seconds. Also, while the timing of variable decelerations in relation to contractions is not a defining component, these decelerations are notably delayed (offset from contractions) in both onset and recovery, a finding that is consistent with late decelerations.
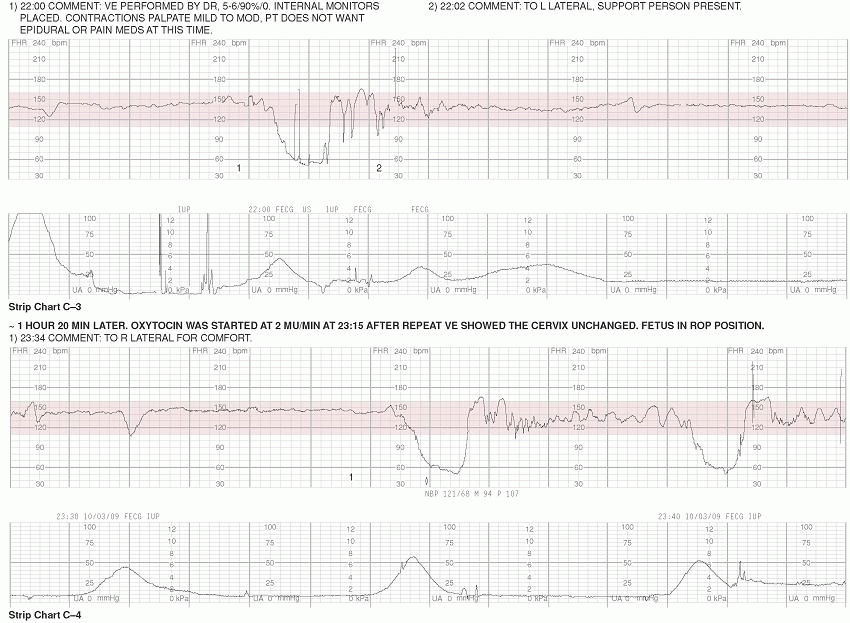
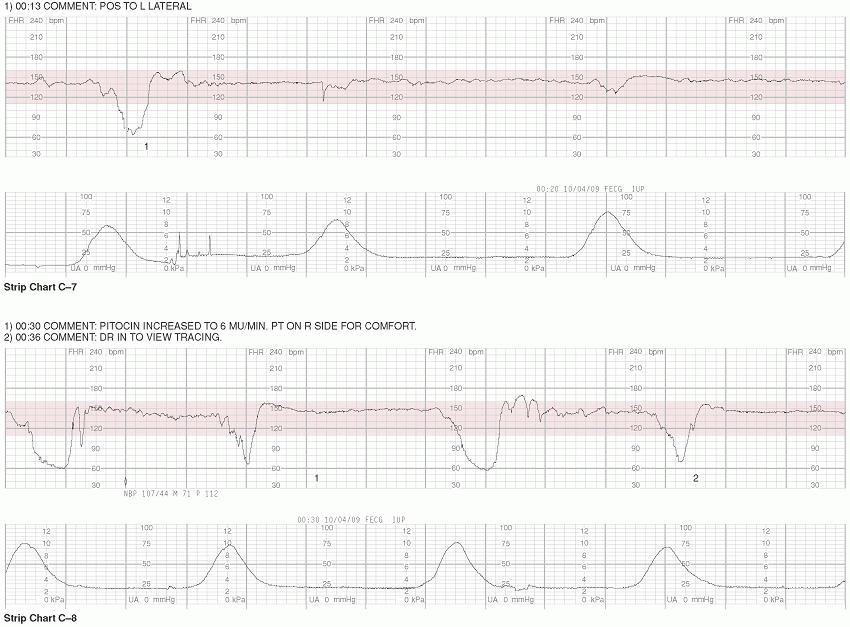
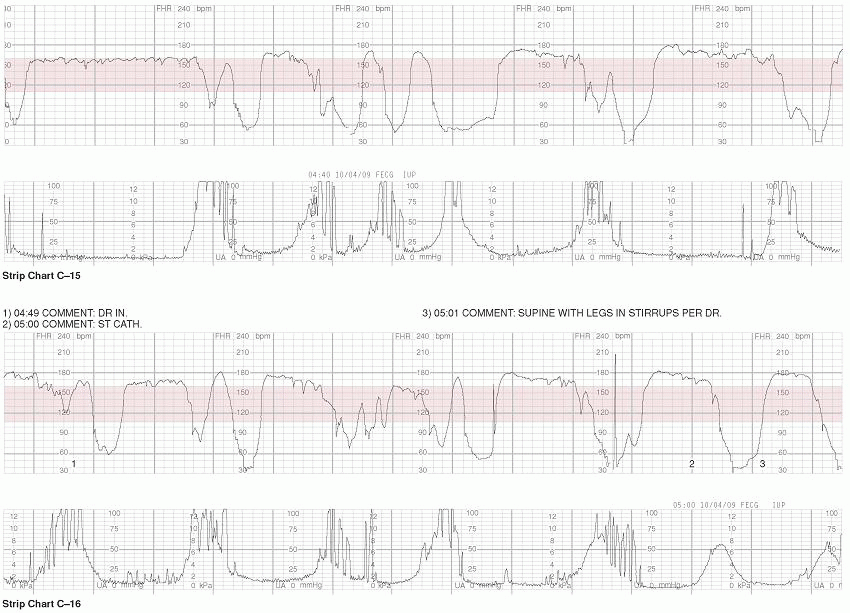
STRIP CHART C-3
Fetal Heart Rate
Uterine Activity
Baseline:
140 bpm
Frequency:
1-3 minutes
Variability:
Minimal
Duration:
1-2.5 minutes
Periodic/Episodic Changes:
Late Decelerations.
Strength:
25-100 mm Hg
Resting Tone:
15 mm Hg
Category:
II
Discussion: With this patient, decelerations seem to be improved with positioning to the left side. Closer observation via internal monitoring was warranted and should assist in determination of fetal status. While this tracing is a Category II, it is pushing the limits of becoming a Category III.
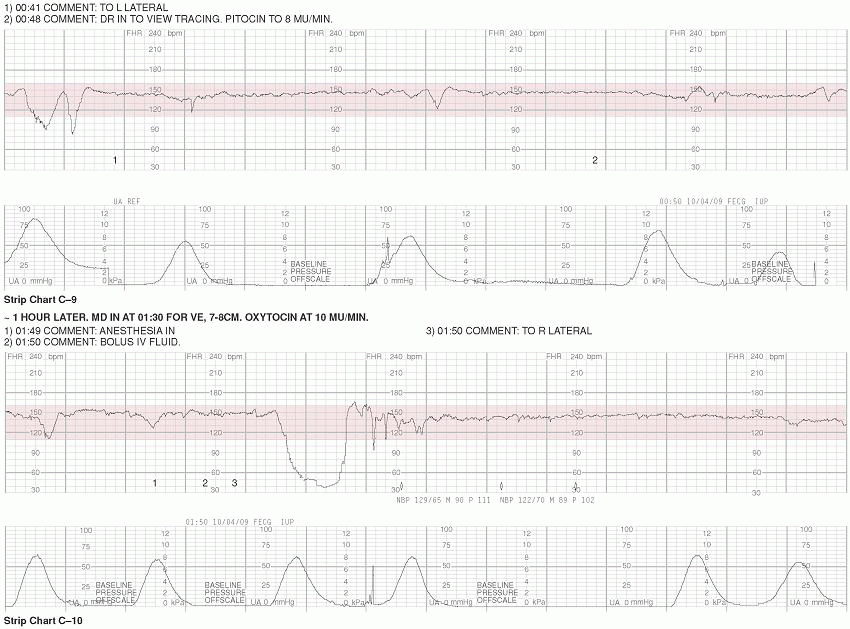
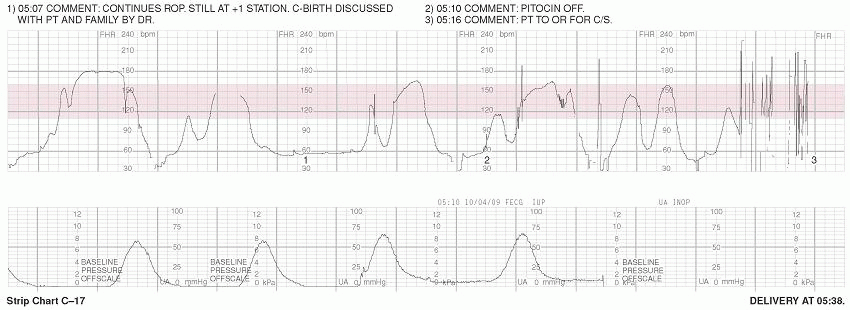
STRIP CHART C-4
Fetal Heart Rate
Uterine Activity
Baseline:
145 bpm
Frequency:
5 minutes
Variability:
Moderate
Duration:
80 seconds-2 minutes
Periodic/Episodic Changes:
Variable and Late Decelerations
Strength:
30-45 mm Hg
Resting Tone:
10 mm Hg
Category:
II
Discussion: After about an hour of no progress with cervical dilation, oxytocin was begun. The fetus is noted to be in a posterior position.
Only gold members can continue reading. Log In or Register to continue