Chapter 485 Epidemiology of Childhood and Adolescent Cancer
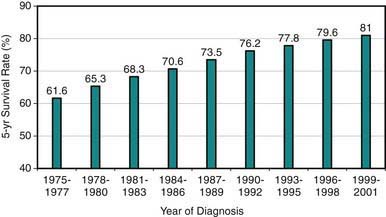
Cancer in patients <19 yr of age is uncommon, with an age-adjusted annual incidence rate of 16.6/100,000, representing only about 1% of all new cancer cases in a year in the USA or 18,000 new cases/yr in 2006. Although relative 5-yr survival rates have improved from 61% in 1977 to 81.6% in 2005 in all age groups (Fig 485-1), malignant neoplasms remain the leading cause of disease-related (noninjury) mortality (12.8%) among persons 1-14 yr of age. There are 1500-1600 cancer-related deaths annually in the USA among children <15 yr of age. The relative contribution of cancer to the overall mortality in 15-19 yr olds is lower. Multi-institutional cooperative clinical trials investigating novel therapies and investigating ways to improve survival rates even further and to decrease treatment-related long-term complications are ongoing. Because increasingly more patients survive their disease, clinical investigation also is focusing on the quality of life among survivors and the late outcomes of therapy experienced by pediatric and adult survivors of childhood cancer. The National Cancer Institute estimates that in 1977 there were 269,700 persons alive (in all age groups) who had survived childhood cancer, corresponding to 1/810 of persons <20 yr of age and 1/1,000 of persons 20-39 yr of age in the US population.
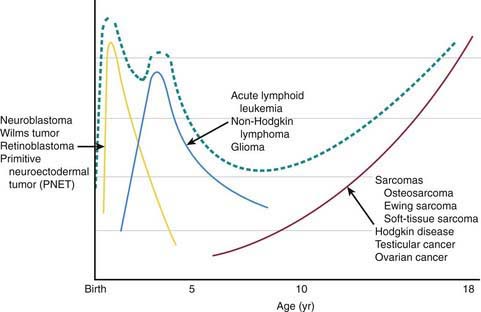
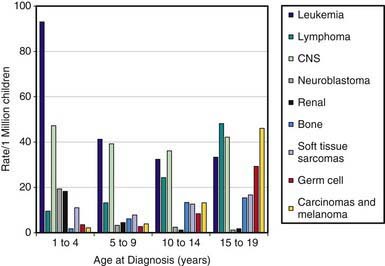
Pediatric cancers differ markedly from adult malignancies in both prognosis and distribution by histology and tumor site. Lymphohematopoietic cancers (i.e., acute lymphoblastic leukemia, lymphomas) account for ~40%, nervous system cancers for ~30%, and embryonal tumors and sarcomas for ~10% each among the broad categories of childhood cancers (Table 485-1). In contrast, epithelial tumors of organs such as lung, colon, breast, and prostate, which are commonly seen among adults, are rare malignancies in children. Unlike incidence patterns in adults, where cancer rates tend to increase rapidly with increasing age, a relatively wide age range exists in the pediatric age group, with 2 peaks: the 1st in early childhood and the 2nd in adolescence (Fig 485-2). During the 1st year of life, embryonal tumors such as neuroblastoma, nephroblastoma, retinoblastoma, rhabdomyosarcoma, hepatoblastoma, and medulloblastoma are most common (Figs 485-3 and 485-4). These tumors are much less common in older children and adults after cell differentiation processes have slowed considerably. Embryonal tumors, acute leukemias, non-Hodgkin lymphomas, and gliomas peak in incidence from 2-5 yr of age. As children age, bone malignancies, Hodgkin disease, gonadal germ cell malignancies (testicular and ovarian carcinomas), and other carcinomas increase in incidence. Adolescence is a transitional period between the common early childhood malignancies and characteristic carcinomas of adulthood (see Fig 485-4).
Table 485-1 AGE-ADJUSTED INCIDENCE AND SURVIVAL RATES OF MALIGNANT NEOPLASMS BY TUMOR TYPE AMONG US CHILDREN
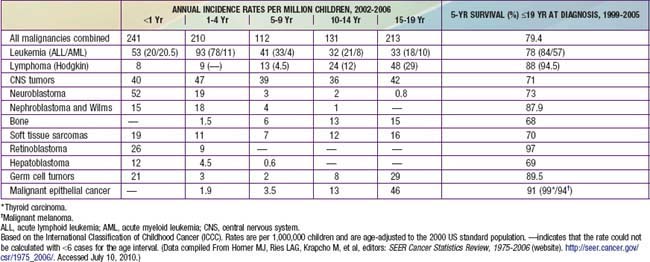
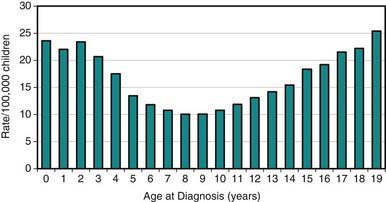
Figure 485-2 Age-specific cancer incidence rates per 100,000 children between 2002-2006 within the USA.
(From Horner MJ, Ries LAG, Krapcho M, et al, editors: SEER cancer statistics review, 1975-2006, Bethesda, MD, 2008, National Cancer Institute.)
(From Horner MJ, Ries LAG, Krapcho M, et al, editors: SEER Cancer Statistics Review, 1975-2006 (website). http://seer.cancer.gov/csr/1975_2006/. Accessed July 10, 2010.)
Childhood neoplasms include a diverse array of malignant tumors, termed “cancers,” and nonmalignant tumors arising from disorders of genetic processes involved in control of cellular growth and development. Although many genetic conditions are associated with increased risks for childhood cancer, such conditions are believed to account for <5% of all occurrences (Chapter 486). The most notable genetic conditions that impart susceptibility to childhood cancer are neurofibromatosis types 1 and 2, Down syndrome, Beckwith-Wiedemann syndrome, tuberous sclerosis, von Hippel-Lindau disease, xeroderma pigmentosum, ataxia-telangiectasia, nevus basal cell carcinoma syndrome, and Li-Fraumeni (p53) syndrome. The varying incidence patterns of individual childhood cancers around the world imply additional genetic and epidemiologic risk factors that remain uncharacterized.
Compared with adult epithelial tumors, an extremely small fraction of pediatric cancers appear to be explained by known environmental exposures (Table 485-2). Ionizing radiation exposure and several chemotherapeutic agents explain only a small number of pediatric cases (Chapter 699
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


