Chapter 16 Endocrine disorders in pregnancy
DIABETES MELLITUS
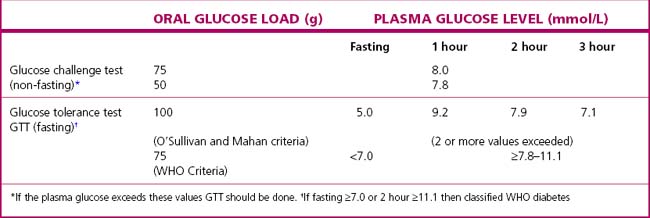
Detection of gestational diabetes
Routine screening of all pregnant women for hyperglycaemia should no longer be considered controversial as two large RCTs have both shown benefit from treating gestational diabetes and the results from the Hyperglycaemia and Adverse Pregnancy Outcome study (HAPO) are being used to define the diagnostic criteria that predict an adverse perinatal outcome. The two currently most widely used criteria are detailed in Table 16.1.
Management of diabetes
Pregnancy
In pregnancy the key principles of management include:
• A multidisciplinary team, including an endocrinologist, a diabetic educator, a dietitian, a neonatologist and obstetrician, is desirable for management.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


