1. Whole limb
2. Humerus
3. Radius
4. Ulna
(a) Mirror hand
(b) Other
5. Digit
(a) Polydactyly
(1) Radial (preaxial, 1st ray, including triphalangeal thumb)
(2) Central
(3) Ulnar (postaxial, 5th ray)
(4) Combinations
6. Epiphyseal (extra)
(a) 1st ray
(b) 2nd ray
(c) Other
This chapter will discuss the various diagnoses that can occur from duplication as well as their treatments, including radial polydactyly, central polydactyly, ulnar polydactyly, and ulnar dimelia (mirror hand).
Radial Polydactyly
Terminology
Radial (preaxial) polydactyly is sometimes called as thumb duplication, split thumb, or bifid thumb. The meaning of “duplication” in the dictionary is “one of two things exactly alike” or “a doubling.” However, it is uncommon in radial polydactyly that the size and shape of the two thumbs are both same and normal. Furthermore, triplication of the thumb was found in 9 out of 121 patients with radial polydactyly in the Netherlands (Zuidam et al. 2008). “Split thumb” has a nuance that it can be a complete thumb if the two components are combined. However, this is not a common situation. “Bifid,” which means “separated into two parts,” may have the same nuance as split thumb. When there is no bony connection between the two thumbs, as in pedunculated type of radial polydactyly, split or bifid thumb may not be an appropriate description. When the parents of a baby with radial polydactyly hear that their baby has a “duplicated,” “split,” or “bifid” thumb, they might simply think that ablation or combination of two parts is enough for surgical treatment.
Although radial polydactyly or polydactyly of the thumb is not a better description for this entity, it just means “many thumbs” which may lessen the misunderstandings of the parents.
Epidemiology
The incidence of radial polydactyly is reported at 0.08–1.4 per 1,000 live births (Sesgin and Stark 1961; Temtamy and McKusick 1978). It is a common congenital difference of the upper extremity in all races, and about 20 % of them occur bilaterally. In Asian countries such as Japan, Korea, and Hong Kong, polydactyly is more common than syndactyly (Ogino et al. 1986; Baek et al. 1997). Syndactyly was more common than polydactyly in the study from University of Iowa (Wassel 1969). Most radial polydactyly occur sporadically. However, when it is associated with triphalangeal thumb, a higher hereditary predisposition has been identified. Radial polydactyly can occur in syndromic diseases such as Fanconi’s anemia, Holt-Oram syndrome, and Rubinstein-Taybi syndrome.
Classification
The Wassel classification for polydactyly of the thumb (Wassel 1969) has been widely used, although several other classification systems have been proposed (Temtamy and McKusick 1978; Chung et al. 2013). This classification system is simple in application and communication (Table 2). Wassel type 4 is the most common type, representing 29–43 % of all polydactyly of the thumb, while type 1 is the least common (Wassel 1969; Al-Qattan 2010).
Type 1: A bifid distal phalanx with a common epiphysis which articulates with a normal proximal phalanx |
There may be one common nail, but usually there are two distinct nails with a groove between them |
Type 2: A completely duplicated distal phalanx |
Each distal phalanx usually has its own epiphysis that articulates with the normal proximal phalanx |
Type 3: A duplicated distal phalanx with a bifurcated proximal phalanx |
The distal phalanges usually diverge from the longitudinal axis, or they may be parallel |
Type 4: A complete duplication of the proximal phalanx |
Each proximal phalanx has its own epiphysis or a common epiphysis that articulates with a normal metacarpal or a metacarpal slightly widened to accommodate both proximal phalanges |
Type 5: A bifurcated first metacarpal |
Each head of the bifurcation articulates with a duplicated proximal phalanx that has its own epiphysis |
Type 6: Complete duplication of the entire first digit |
One side may be more rudimentary than the other |
Type 7: A triphalangeal thumb or elements of a triphalangeal thumb accompanied by a normal thumb |
The Wassel classification is based on an assessment of the skeleton. In young children whose skeleton is immature, the true nature of the thumbs may not be apparent. For instance, Wassel type 1 polydactyly can be classified as a type 2 until ossification of the distal phalangeal epiphysis becomes apparent (Tonkin 2012). Wassel type 7 polydactyly which has a triphalangeal component shows diverse manifestations and is further subclassified into six types (Wood 1978).
There are some types of radial polydactyly unclassifiable by the Wassel system. Pedunculated type, triplicated thumb, or extra thumb that does not have bony connection with the main thumb cannot be classified.
Preoperative Evaluation and Discussion with the Parents and Patient
When a baby with radial polyactyly and his/her parents visit the outpatient department (OPD), it is important to inspect both hands of the patient. Most of the babies with unilateral involvement show smaller sizes of affected thumbs than those of contralateral normal thumbs. Thus, the parents should understand that even if the more dominant one is preserved in the affected thumb, it will be smaller in length and girth when compared to the unaffected side.
In babies with bilateral involvement, the nail size of index finger can be a reference to judge the size of the affected thumbs. The width of the index finger nail is about two thirds of that of the thumb in normal babies.
Active motion of each joint is hard to observe because the babies usually clench their hands. Passive motion and varus and valgus stress tests of the joints, palpation of tendons (especially flexor tendons), and observation of skin crease may be helpful to evaluate the polydactylic thumbs. Little or absent passive motion at bifurcation site of minor thumb (mostly radial one) may suggest odd numbered Wassel type 1, 3, or 5. It is much easier to reconstruct a thumb that has stable joints in radioulnar plane. If the flexor tendon is palpable while moving the joint passively, good active motion can be expected postoperatively. When the skin crease is faint or absent, there is a strong possibility that the affected joint does not have effective motor power.
Simple radiographs are a prerequisite for Wassel typing and surgical planning. Although it is not easy to obtain a true PA and lateral view of the affected thumbs, it is absolutely necessary for surgical planning. Radiographs of normal side in unilateral cases are also important in assessing the size and shape of bones and joints of the affected thumbs comparatively. Medical photos are also needed for documentation and later evaluation of surgical outcome.
Before surgery, the parents should be informed that even if the thumb is successfully reconstructed, it will not be the same as the contralateral normal thumb in terms of function and appearance.
In a study of 66 years of experiences for surgery of the duplicated thumb (Townsend et al. 1994), there were 52 % of patients with unacceptable results, 18 % of them unsalvageable by secondary surgery. More recently, the complication rates appear to be lowering. When initial surgery was planned to restore all anatomic elements, the need for secondary surgery was unusual (Waters and Bae 2012, p. 41). The primary issues affecting appearance after surgery for radial polydactyly were reduced nail width and angulation at interphalangeal joint. Reconstructed Wassel type 7 thumbs had lower satisfaction score than other types (Goldfarb et al. 2008). The patients and their parents sometimes complain of the postoperative long arm cast; however, a short arm cast can be easily removed in young children.
Timing of Surgery
There has been no consensus on the timing of operation for radial polydactyly. In the textbook of Green’s operative hand surgery, it is recommended to perform surgery at about 1 year of age before the development of thumb-index finger pinch (Kozin 2011). In the textbook of Campbell’s operative orthopedics, it is recommended to perform surgical reconstruction when the child is about 18 months old, but no later than 5 years old if possible (Jobe 2011). Indebted to recent advancement in pediatric anesthesia, most surgeries can be performed safely if the patient does not have serious comorbidity, such as cardiac anomaly or pancytopenia. In certain cases, Wassel type 7, for example, bony shape of the delta bone, is sometimes important for surgical planning in which the surgical timing is better to be postponed until it is clearly visible in radiographs. Thus, timing of surgery depends on general condition of the patients, priority of surgery in patients with multiple associated anomalies, types of radial polydactyly, and equally importantly surgeon’s preference. There is no gold standard for surgical timing of radial polydactyly. However, earlier surgery is recommended when surgical planning is completed and the structures of the thumb are large enough to manipulate surgically.
The same principles of timing of surgery can be applied to central polyactyly and ulnar polydactyly.
Surgical Techniques
The goal of surgical reconstruction is to make a straight, mobile, and stable thumb of good appearance in size and shape. However, there is no hand surgeon that can make a normal thumb. We are trying to make a better thumb in a given situation, not the best or perfect thumb.
The patients with radial polydactyly show diverse manifestations, from a rudimentary floating type to a complex one. Ligation or simple excision may be enough for floating types of radial polydactyly. However, simple ablation of one digit has not produced satisfactory outcomes in most cases of radial polydactyly. Resultant deviation, stiffness, and/or ligamentous instability of the thumb is commonplace. Although surgical concepts and techniques are still evolving, there are several reconstructive strategies to achieve a functionally and aesthetically acceptable thumb.
Surgical techniques to reconstruct radial polydactyly can be classified into five types – ligation, simple excision, excision and reconstruction, combination procedures (Bilhaut-Cloquet operation), and on-top plasty.
Radial polydactyly |
|---|
Surgical techniques |
Ligation |
Simple excision |
Excision and reconstruction |
Combination procedure (Bilhaut-Cloquet operation) |
On-top plasty |
The surgical wound is usually closed with absorbable 5-0 or 6-0 sutures. If the wound is closed with nonabsorbable sutures, sedation of the patients may be needed for stitch removal. A long arm thumb spica cast with more than 90° of elbow flexion is recommended postoperatively, because a short arm thumb spica cast or a long arm cast in a position of less elbow flexion can be easily taken off. Duration of immobilization for patients undergoing corrective osteotomy and/or reconstruction of collateral ligament should be 4–6 weeks depending on the patient age. Postoperative therapy is not necessary in most patients.
Radial polydactyly | |
|---|---|
Operative treatment | |
Surgical techniques | Indications |
Ligation | Pedunculated type |
Simple excision | No bony connection between two polydactyly thumbs. Dominant thumb shows good stability, motion, and appearance |
Excision and reconstruction | Most of radial polydactyly |
Combination procedure | Both thumbs are hypoplastic and almost symmetric, especially, when the nail width is less than 2/3 of contralateral normal side in unilateral cases and when the nail width is less than that of index finger in bilateral cases |
On-top plasty | One thumb has well-developed proximal part and poorly developed distal part with absent or hypoplastic nail. The other thumb has poorly developed proximal part and better distal part including nail and pulp |
Ligation
In a pedunculated type of radial polydactyly, ligation at the base as close as possible to its root with 5-0 or 6-0 Nylon with or without local anesthesia can be performed in the outpatient department or nursery (Fig. 1). A ligated hypoplastic thumb will mummify and usually falls off within 2 weeks (Fig. 2). A nubbin or dimple usually remains afterward (Fig. 3). Even in pedunculated type of polydactyly, painful neuroma may develop after the ligation, which is an indication for surgical exploration (Leber and Gosain 2003).



Fig. 1
A pedunculated and partly necrotic radial polydactyly of a newborn baby. Vascular structures are seen in the stalk
Fig. 2
Ligated thumb became mummified and fell off 9 days after the ligation
Fig. 3
An asymptomatic dimple is remained after the ligation
Simple Excision
When there is no bony connection between two polydactyly thumbs and a dominant thumb shows good stability, motion, and appearance, simple excision under general anesthesia is indicated (Figs. 4, 5, and 6).



Fig. 4
A minor radial thumb is attached to the robust main thumb
Fig. 5
There was no bony connection between two thumbs
Fig. 6
Good appearance after simple excision
Technique: An elliptical incision is made around the minor thumb. The soft tissue pedicle usually contains neurovascular structures. To avoid bleeding, the vessels should be ligated or cauterized. To prevent painful neuroma, the nerve should be identified, sharply transected, and embedded in the soft tissue.
Excision and Reconstruction
Most of radial polydactyly can be successfully treated by the “excision and reconstruction” technique (Fig. 7). Main components of this procedure are arthroplasty, corrective osteotomy, and tendon realignment. When one of the two polydactylic thumbs is well developed and the other one less developed, this technique is indicated. However, when both polydactylic thumbs are hypoplastic, this technique results in a small thumb which is sometimes smaller than the index tip. Surgical technique for Wassel types 1 and 2 is similar. Also similar surgical technique can be applied to Wassel types 3, 4, 5, and 6. For the diversity of clinical features, surgical technique for Wassel type 7 should be individualized case by case.
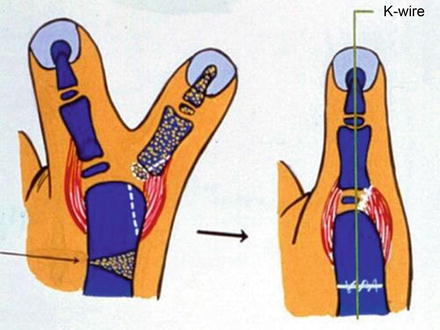
Fig. 7
Ligamentoperiosteal flap was raised to reconstruct radial collateral ligament of MP joint. Metacarpal head was excised partially to fit base of dominant proximal phalanx. Corrective osteotomy was added to make a straight thumb
Arthroplasty: Arthroplasty consists of joint stabilization by ligamentoperiosteal flap (Manske 1989) and partial excision of excessive portion of phalangeal or metacarpal head that articulates with the two thumbs.
Two thumbs articulate with a single proximal phalangeal head in Wassel type 1 or 2 radial polydactyly and on a single metacarpal head in type 3 or 4. During dissection of minor thumb, distal insertion of collateral ligament should be preserved with adjacent periosteal tissue for later reconstruction. This ligamentoperiosteal flap is reattached to base of phalangeal bone of the retained main thumb after removal of the minor thumb. The phalangeal or metacarpal head, when minor thumb is removed, is relatively large for the remained dominant thumb. This size mismatching may cause angular deformity and/or bony prominence if it is not corrected. Thus, excessive portion of the head needs to be shaved or removed. Sometimes, a separate facet that articulates with the radial thumb to be deleted is observed. This facet can be used as a guideline to cut excessive portion. Conventional oscillating saw or osteotomes cannot be used for small phalangeal bones of young children. Their phalangeal bones are soft enough that shaving of articular cartilage and partial ostectomy can be performed by a small rongeur or a No. 15 surgical blade. Excessive tension of the reconstructed collateral ligament to correct angular deformity at the joint level is not recommended because the deformity is likely to recur and stiffness of the joint may occur. However, angular deformity of less than 10° at the joint level can be corrected by this arthroplasty procedure. A longitudinal Kirschner wire (K-wire) is inserted to protect the reconstructed collateral ligament.
Corrective Osteotomy: Angulation at interphalangeal joint and reduced nail width are primary issues affecting appearance after the surgery (Goldfarb et al. 2008). More than 20° of angular deformity is not acceptable to most patients and parents. The angulation can be corrected by closed wedge osteotomy. Double-level osteotomy at proximal phalangeal and metacarpal levels can be indicated to align severe divergent-convergent Wassel type 4.
Tendon Realignment: Abnormal insertions of flexor pollicis longus (FPL) and/or extensor pollicis longus (EPL) are not uncommon in radial polydactyly, especially in Wassel type 4. The FPL tendon attaches not only at its customary insertion but also into the extensor by a tendon that passes around the radial aspect of the thumb. This anomalous muscle abducts the thumb instead of flexion and is called as pollex abductus (Tupper 1969; Lister 1991). The abnormal alignment of FPL and/or EPL may cause gradual angular deformity even after successful bony alignment has been achieved by corrective osteotomy. When there are abnormal insertions of FPL and/or EPL tendons, the insertion sites should be realigned to achieve a good flexion-extension arc. The abnormal insertion can be completely detached and reattached into the correct position. The phalangeal bones of young children are soft that the tendon can be sutured into the distal phalanx using 4-0 or 5-0 Nylon. When the phalangeal bone is too hard to be sutured by Nylon suture, a pullout suture technique can be used. When the distal portion of the tendon is bifid and inserted into both polydactylic thumbs, it usually inserts at ulnar side of the radial thumb and radial side of the ulnar thumb. If the radial thumb is to be removed, the tendon is detached from the insertion of radial thumb and reattached into the ulnar side of dominant ulnar thumb like Y shape to balance the vector forces (Figs. 8 and 9).
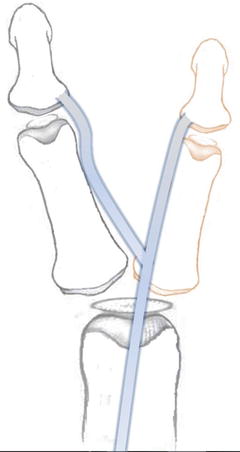

Fig. 8
The tendons frequently bifurcated distal to the MP joint, and insert to the side of each distal phalanx
Fig. 9
The tendon insertion of minor thumb is detached and reattached to the main thumb in Y shape to balance the vector force
In Wassel type 4, 5, 6, or 7 polydactyly of the thumb, some of thenar muscles insert into the radial side thumb. In most cases, the radial thumb is removed and the ulnar thumb is reconstructed. The insertion site of thenar muscles on the radial thumb should be identified and dissected carefully for later reattachment to the main ulnar thumb.
Excision and reconstruction |
|---|
Surgical components |
Arthroplasty: joint stabilization by ligamentoperiosteal flap and partial excision of excessive portion of phalangeal or metacarpal head |
Corrective osteotomy for angular deformity |
Tendon realignment when FPL/EPL insertions are abnormal |
Surgical Technique (Wassel Type 2): A 9-month-old boy showed hypoplastic Wassel type 6 radial polydactyly on right thumb and Wassel type 2 on left (Fig. 10). The nail size, length, and girth of ulnar side thumb of left hand were good enough to perform the “excision of radial thumb and reconstruction” procedure. Although the epiphyses of phalanges and metacarpal are not observed in simple radiograph (Fig. 11), it is easy to decide the surgical plan as “arthroplasty” with or without “tendon realignment.” Corrective osteotomy will not be necessary because angular deformity at the IP joint is minimal. A racquet-shaped incision was designed (Fig. 12). A zigzag incision has an advantage to prevent possible scar contracture, but this technique is not easy to apply to a small-sized thumb less than an inch in length in infant age. The dissection was deepened to expose distal phalangeal bone of the radial thumb, and a ligamentoperiosteal flap was raised using No. 15 blade (Fig. 13). Distal phalanx of the radial thumb was cut to be removed, and articular surface of this radial thumb was seen (Fig. 14). Articular surface for the radial thumb was cut using No. 15 blade (Fig. 15). The consistency of phalangeal bone in infant age is soft enough to be cut by surgical blade. There was no malalignment of tendon found. After the arthroplasty procedure, the articular surface of the proximal phalanx fit that of ulnar thumb (Fig. 16). Before reconstruction of the collateral ligament, a 0.7 mm K-wire was inserted longitudinally to protect it. The ligamentoperiosteal flap for reconstruction of the collateral ligament was attached to the new insertion site by 5-0 absorbable suture (Fig. 17). Direct suture of skin edge to the nail does not achieve normal lateral nail fold. A suture needle was introduced about 3 mm away from the skin flap to be sutured to the nail, and it came out 1 mm away from the skin flap to simulate the lateral nail fold. Then the needle was passed through the nail, and tied (Fig. 18). The reconstructed thumb looked straight and reconstructed lateral nail fold looked adequate (Fig. 19). On a postoperative radiograph, shaved proximal phalangeal head fit distal phalanx so well that IP joint looked natural (Fig. 20).



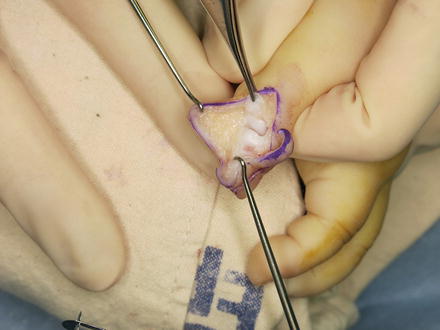

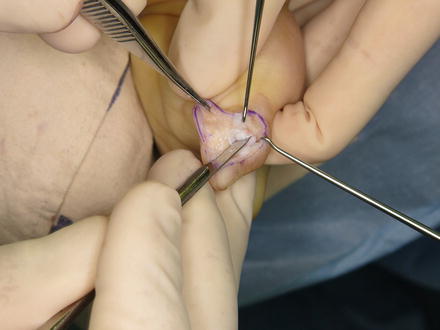





Fig. 10
Wassel type 2 polydactyly of left thumb
Fig. 11
Ulnar distal phalanx showed better configuration
Fig. 12
Skin incision
Fig. 13
A ligamentoperiosteal flap was raised (forcep)
Fig. 14
The articular surface for removed radial distal phalanx was observed
Fig. 15
This portion was cut using No. 15 blade
Fig. 16
Now the articular surfaces of the IP joint fit very well
Fig. 17
A K-wire was inserted longitudinally, and the flap was reattached to the new insertion site
Fig. 18
To simulate lateral fold of the nail, suture needle was introduced about 3 mm away from the skin flap, and it came out 1 mm away from the skin flap and then passed through the nail
Fig. 19
The lateral nail fold looked natural after reconstruction
Fig. 20
Shaved proximal phalangeal head fit distal phalanx on a postoperative radiograph
Surgical Technique (Wassel Type 4): An 11-month-old boy showed a divergent-convergent Wassel type 4 radial polydactyly. The radial thumb of left hand was hypoplastic, but the ulnar thumb showed good size and shape (Fig. 21). There was 40° of angular deformity at the IP joint of ulnar thumb that needed corrective osteotomy at proximal phalangeal neck level (Fig. 22). Medical photos and simple radiographs suggested strong possibility that arthroplasty of MP joint and tendon realignment of EPL, FPL, and thenar muscles were necessary for proper reconstruction. Proximal phalangeal head of the ulnar thumb was underdeveloped, suggesting a potential recurrence of angular deformity postoperatively. A racquet-shaped incision was designed (Fig. 23). The EPL tendon was bifurcated at MP joint level and inserted into both thumbs. The insertion site of radial EPL slip was detached (Fig. 24) and sutured to the ulnar side of dominant thumb to balance the extension force (Fig. 25). The FPL tendon showed the same pattern. The insertion site of radial FPL slip was detached and tagged with suture for later reattachment into the ulnar side of dominant thumb (Fig. 26). The abductor pollicis brevis muscle insertion into the radial thumb was detached from the proximal phalangeal base for later reattachment into the reconstructed thumb. The radial thumb was removed leaving ligamentoperiosteal flap for later reconstruction of the MP joint. The portion of metacarpal head to be resected was lined, and a ligamentoperiosteal flap was raised and preserved (Fig. 27). Excessive portion of articular cartilage and bone was removed by No. 15 blade and small osteotomes (Fig. 28). Then proximal phalanx was dissected subperiosteally for an ulnar-based closed wedge osteotomy to correct angular deformity at the IP joint (Fig. 29). It is convenient to perform ulnar-based closed wedge osteotomy from ulnar side incision. However, simultaneous medial and lateral incision on the same thumb may jeopardize blood circulation. The MP joint was fixed in a reduced position with a K-wire, and also osteotomy site of proximal phalanx was fixed with an additional K-wire (Fig. 30). Finally the FPL tendon detached from the radial thumb was reattached into the ulnar side of reconstructed distal phalanx. The abductor pollicis brevis tendon detached from radial thumb as well as the previously raised ligamentoperiosteal flap for collateral ligament reconstruction was reinserted into the base of proximal phalanx (Fig. 31). Alignment and appearance of the reconstructed thumb (Fig. 32) and the immediate postoperative radiograph (Fig. 33) showed reasonable result.




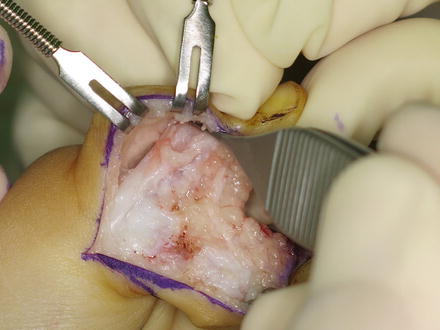


Fig. 21
Wassel type 4 radial polydactyly of an 11-month old boy
Fig. 22
The ulnar side thumb showed better bony development, although there was 40° of angular deformity at the IP joint
Fig. 23
Skin incision
Fig. 24
The EPL tendon to the radial thumb was detached
Fig. 25
The detached tendon was sutured to the ulnae side of ulnar thumb
Fig. 26
The FPL insertion to the radial thumb was identified and tagged with suture for later reattachment
Fig. 27




Excessive portion of metacarpal head on which the removed radial thumb sit was marked. A ligamentoperiosteal flap was raised from radial proximal phalanx (left skin hook)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
