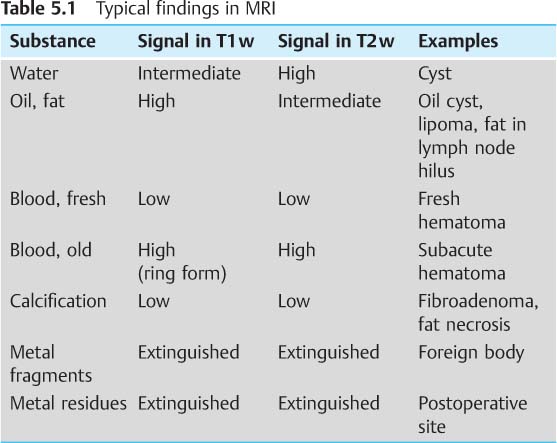
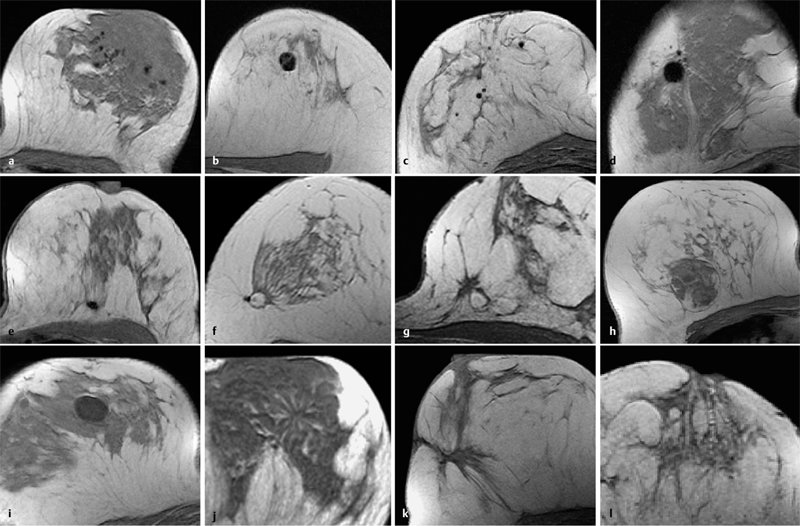
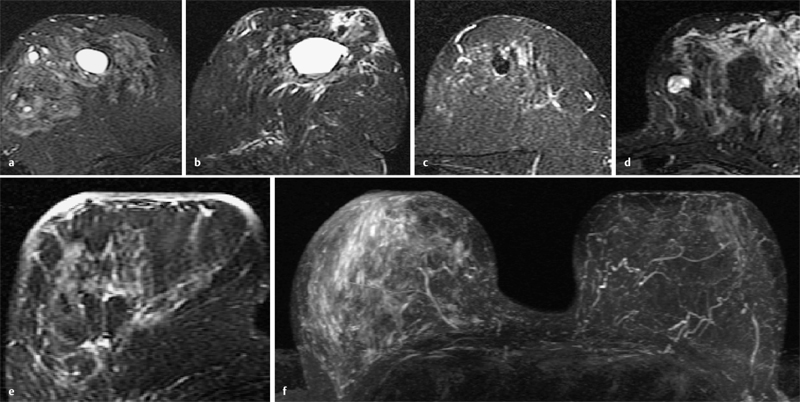
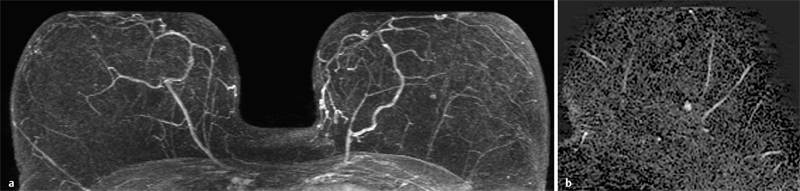
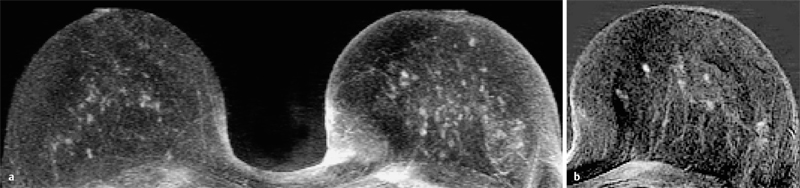
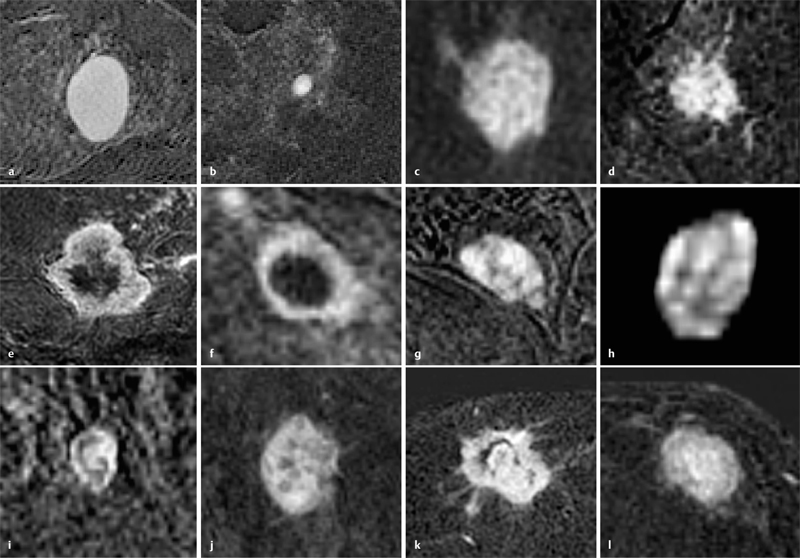
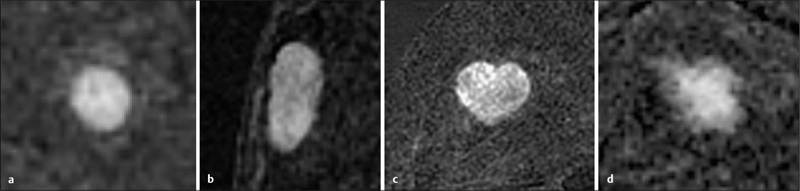
5 Diagnostic Criteria As in other areas of imaging-based diagnostics, the evaluation of a breast MRI examination entails both the detection and also the characterization of suspicious lesions. High-quality MRI technique and methodology are necessary to depict hypervascularized changes reliably and free of artifacts, and are prerequisites for the detection of relevant breast lesions. Once detected, hypervascularized findings must be substantiated and characterized according to morphological and dynamic contrast criteria. Here, the personal expertise of the examiner is of great importance. In certain constellations, the T1w precontrast examination can provide important additional information that sometimes permits a better interpretation of MRI findings. Especially notable are architectural distortions, peritumoral structural changes, fatty inclusions within ambiguous lesions, and therapy-induced and/or artificial changes (Table 5.1 and Fig. 5.1). However, the reliable detection of breast cancer and adequate differentiation between benign and malignant tumors cannot be achieved without the intravenous administration of contrast. a Spotty signal-free areas (diffuse, intramammary macrocalcifications). b Endotumoral signal-free region (macrocalcification within a regressive fibroadenoma). c Punctate, round signal extinction (susceptibility artifacts due to electrocautery during surgery). d Large round signal extinction (susceptibility artifacts due to broken needle tip). e Small oval signal extinction (susceptibility artifact due to clip marking). f Round lesion with high signal intensity surrounded by signal-free zone (calcified oil cyst). g Lesion with high signal intensity after vacuum biopsy (blood in resection cavity). h Encapsulated space-occupying lesion with inhomogeneous internal signal intensity (hamartoma). i Smooth-bordered, homogeneous lesion with low signal intensity (e. g., cyst, fibroadenoma). j Architectural distortion within breast parenchyma (e.g., radial scar, tubular carcinoma). k Hypointense architectural distortion showing retraction of surrounding tissue (postoperative scar). l Increased signal intensity within retromamillary ducts (lactation phase). In T2w imaging, water has a very high signal intensity. The supplementary evaluation of these images allows a better assessment of hypervascularized lesions (Fig. 5.2). In addition, internal septations, which are a characteristic feature of myxoid fibroadenomas, are often best visualized in the T2w images. Fig. 5.2a–f Relevant findings in T2w images (IR with fat suppression). a Oval, smooth-bordered lesion with very high signal intensity (cyst). b Lesion with very high signal intensity and parietal areas with lower signal intensity (seroma). c Hypointense round lesion (fibrous fibroadenoma). d Hypointense septations within hyperintense lesion (myxoid fibroadenoma). e Global skin thickening with high signal intensity (after breast radiotherapy). f Asymmetric, diffuse increase of signal intensity in the right breast (after radiotherapy of the right breast). The assessment of hypervascularized structures in breast MRI is generally performed using the early subtraction slice images. If the breast parenchyma shows strong enhancement in this phase of the examination, the supplementary assessment of the earliest subtraction images may be more useful. In accordance with the ACR BI-RADS–MRI Lexicon, three types of lesions can be differentiated: The following description of each type of enhancing lesion includes illustrative image examples. A focus is a tiny spot of unspecific enhancement whose morphology cannot be characterized further due to its small size, and which has no corresponding structure on the T1w precontrast image (Fig. 5.3). Foci are multiple, tiny, circumscribable enhancing areas (Fig. 5.4). Typically, a focus is smaller than 5 mm in diameter. A mass is a three-dimensional, space-occupying lesion that either displaces or has some other influence on the surrounding tissues. Fig. 5.3a, b Focus. a MIP of subtraction images shows a solitary, hypervascularized lesion with a diameter of 3 mm (focus) in the central aspect of the left breast. b The same focus in a subtraction slice image. Fig. 5.4a, b Foci. a MIP of subtraction images shows multiple, finely speckled hypervascularized areas with a maximum diameter of 4 mm (foci) in both breasts. b Representative subtraction slice image. Fig. 5.6a–c Margins of hypervascularized mass lesions. a Well-circumscribed/smooth. b Irregular. c Spiculated. The shape of a contrast-enhancing region in the subtraction image describes its spatial form. A round, oval, or lobulated shape usually designates a benign lesion, whereas a lesion with an irregular shape has a greater probability of malignancy (Fig. 5.5). Shape of Contrast-Enhancing Lesion The margins of a contrast enhancing region in the subtraction image describe its outer contours. Smooth, well-defined margins usually designate a benign lesion. Irregular margins or spiculations extending into the parenchyma designate a greater probability, but are not proof of malignancy (Fig. 5.6). Margins of Contrast-Enhancing Lesions The contrast enhancement pattern describes the spatial distribution of contrast within the contrast-enhancing lesion (internal enhancement). Internal Patterns of Contrast-Enhancing Mass Lesions Homogeneous, inhomogeneous, rim-enhancement. A homogeneous internal contrast enhancement pattern in a mass lesion is usually indicative of a benign proliferating process. An inhomogeneous internal contrast enhancement pattern is considered unspecific. Because a carcinoma has its biologically active zone in the tumor periphery, however, a rim-enhancement pattern can correspond to an increased perfusion of these areas relative to the tumor center and must be considered suspicious for malignancy. Septations, central enhancement. Internal, hypovascularized septations are a reliable criterion for myxoid fibroadenomas. Great caution is recommended, however, because wide septations in the center of a fibroadenoma are occasionally very difficult to differentiate from a rim-enhancement associated with carcinomas. Hypervascularized internal septations, on the other hand, are an indication of an increased proliferation rate and must always prompt one to include malignancy in the differential diagnosis. This is also true when a central region with increased vascularization is seen within a mass lesion (Fig. 5.7). Fig. 5.7a–l Internal contrast enhancement patterns within hypervascularized mass lesions. a, b Homogeneous. c, d Heterogeneous. e Rim-enhancement (thick rim). f Rim-enhancement (thin rim). g, h Dark internal septations (not enhancing). i, j Enhancing internal septations. k, l Central enhancement.
Assessment of the T1-Weighted Precontrast Examination
 In T1w precontrast images, structures with a high signal intensity correspond to fat, protein, or blood.
In T1w precontrast images, structures with a high signal intensity correspond to fat, protein, or blood.
Assessment of the T2-Weighted Examination
 Internal septations are characteristic features of myxoid fibroadenomas and are frequently best visualized in the T2w images.
Internal septations are characteristic features of myxoid fibroadenomas and are frequently best visualized in the T2w images.
Assessment of the Contrast-Enhanced T1-Weighted Examination
 Focus/foci
Focus/foci
 Mass
Mass
 Nonmasslike enhancement
Nonmasslike enhancement
Focus/Foci
Mass
 The morphological criteria of a mass are its shape, margin, and enhancement pattern.
The morphological criteria of a mass are its shape, margin, and enhancement pattern.
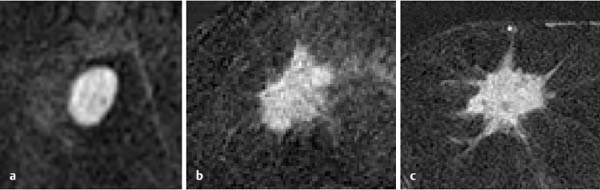
Shape
 Round
Round
 Oval
Oval
 Lobulated
Lobulated
 Irregular
Irregular
Margins
 Well-defined, smooth
Well-defined, smooth
 Irregular
Irregular
 Spiculated
Spiculated
Enhancement Pattern
 Homogeneous
Homogeneous
 Heterogeneous
Heterogeneous
 Peripheral enhancement (rim sign)*
Peripheral enhancement (rim sign)*
 Dark internal septations
Dark internal septations
 Enhancing internal septations
Enhancing internal septations
 Central enhancement
Central enhancement
Diagnostic Criteria
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


