Chapter 94 Delivery Room Emergencies
Most infants complete the transition to extrauterine life without difficulty; however, a small percentage requires resuscitation after birth. The most common delivery room emergency for neonates is secondary to failure to initiate and maintain effective respirations. Less frequent, but of major importance, are shock (Chapter 92), severe anemia (Chapter 97.1), plethora (Chapter 97.3), convulsions (Chapter 586.7), and management of life-threatening congenital malformations (Chapter 92). Improved perinatal care and prenatal diagnosis of fetal anomalies allow for appropriate maternal transports for high-risk deliveries.
Respiratory Distress and Failure
Disorders of respiration in newborn infants can be categorized as either central nervous system (CNS) failure, representing depression or failure of the respiratory center, or peripheral respiratory difficulty, indicating interference with the alveolar exchange of oxygen and carbon dioxide. Cyanosis occurs in both groups (see Table 92-1). Respiratory problems encountered in the delivery room are most frequently those of airway obstruction and depression of the CNS (maternal medications, asphyxia) with an absence of adequate respiratory effort. Respiratory distress in the presence of good respiratory effort should lead to an immediate consideration of the underlying cause and is an indication for radiographic examination of the chest.
If respiratory movements are made with the mouth closed but the infant fails to move air in and out of the lungs, bilateral choanal atresia (Chapter 368) or other obstruction of the upper respiratory tract should be suspected. The mouth should be opened, and the mouth and posterior of the pharynx cleared of secretions with gentle suction. An oropharyngeal airway should be inserted, and the source of the obstruction sought immediately. If effective respiratory flow is not produced by opening the infant’s mouth and clearing the airway, laryngoscopy is indicated. With obstructive malformations of the mandible, epiglottis, larynx, or trachea, an endotracheal tube should be inserted; prolonged endotracheal intubation or tracheostomy may be required. Respiratory failure caused by CNS depression or injury may require continuous mechanical ventilation.
Hypoplasia of the mandible (Pierre Robin, DiGeorge, and other syndromes; Chapters 300 and 303) with posterior displacement of the tongue may result in symptoms similar to those of choanal atresia and may be temporarily relieved by pulling the tongue or mandible forward or placing the infant in the prone position. A scaphoid abdomen suggests a diaphragmatic hernia or eventration, as does asymmetry in contour or movement of the chest or a shift of the apical impulse of the heart; these latter manifestations are also compatible with tension pneumothorax. A pneumothorax can be the presenting symptom in infants with pulmonary hypoplasia, renal malformations, or both.
Pulmonary causes of respiratory difficulty are discussed in Chapter 95.
Neonatal Resuscitation
Immediately after birth, an infant in need of resuscitation should be placed under a radiant heater and dried (to avoid hypothermia), positioned with the head down and slightly extended; the airway should be cleared by suctioning, and gentle tactile stimulation provided (slapping the foot, rubbing the back). Simultaneously, the infant’s color, heart rate, and respiratory effort should be assessed (Fig. 94-1).
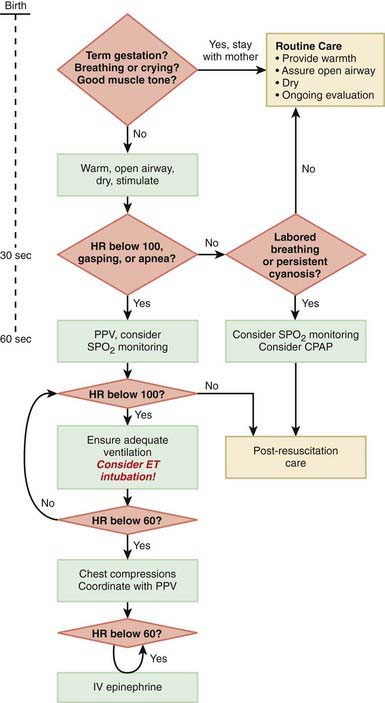
The steps in neonatal resuscitation follow the ABCs: A, anticipate and establish a patent airway by suctioning and, if necessary, performing endotracheal intubation; B, initiate breathing by using tactile stimulation or positive-pressure ventilation with a bag and mask or through an endotracheal tube; C, maintain the circulation with chest compression and medications, if needed. Steps to follow for immediate neonatal evaluation and resuscitation are outlined in Figure 94-1 (Chapter 62).
If no respirations are noted or if the heart rate is <100 beats/min, positive pressure ventilation is given through a tightly fitted face bag and mask for 15-30 sec. In infants with severe respiratory depression that does not respond to positive-pressure ventilation via bag and mask, endotracheal intubation should be performed. Many authorities recommend early intubation for extremely low birthweight (ELBW) preterm infants. Guidelines for endotracheal tube size and depth of insertion in infants with different birthweights are shown in Table 94-1. If the heart rate does not improve after 30 sec with bag and mask (or endotracheal) ventilation and remains below 100 beats/min, ventilation is continued and chest compression should be initiated over the lower third of the sternum at a rate of 120 beats/min. The ratio of compressions to ventilation is 3:1. If the heart rate remains <60 beats/min despite effective compressions and ventilation, administration of epinephrine should be considered. Persistent bradycardia in neonates is usually due to hypoxia resulting from respiratory arrest and often responds rapidly to effective ventilation alone. Persistent bradycardia despite what appears to be adequate resuscitation suggests more severe cardiac compromise or inadequate ventilation technique. Poor response to ventilation may be due to a loosely fitted mask, poor positioning of the endotracheal tube, intraesophageal intubation, airway obstruction, insufficient pressure, pleural effusions, pneumothorax, excessive air in the stomach, asystole, hypovolemia, diaphragmatic hernia, or prolonged intrauterine asphyxia.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


