Cystic Abdominal Mass
Alexander J. Towbin, MD
DIFFERENTIAL DIAGNOSIS
Common
Hydronephrosis
Ovarian Cyst
Multicystic Dysplastic Kidney
Pancreatic Pseudocyst
Appendiceal Abscess
Duplication Cyst
Less Common
Splenic Cyst
Urachal Cyst
Hydrometrocolpos
Choledochal Cyst
Cystic Wilms Tumor
Rare but Important
Meconium Pseudocyst
Multilocular Cystic Nephroma
Mesenchymal Hamartoma
Caroli Disease
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Organ of origin can be difficult to identify for large cystic masses
Most cystic masses have renal origin
Patient age and mass location can focus differential diagnosis
Helpful Clues for Common Diagnoses
Hydronephrosis
Most common pediatric abdominal mass
Diagnosed in 1-5% of pregnancies
Up to 30% are bilateral
Resolves on postnatal US in ˜ 50%
10% have ureteropelvic junction (UPJ) obstruction
Vesicoureteral reflux in 10%
Postnatal US should be 1st imaging test
Hint: Consider posterior urethral valves in males with bilateral hydronephrosis
Ovarian Cyst
Most common during infancy and adolescence
Fetal cysts more common with maternal diabetes, toxemia, and Rh isoimmunization
At birth, up to 98% of girls have small ovarian cysts
20% of neonatal cysts > 9 mm
Neonatal cysts resolve spontaneously
Cysts resolve as maternal hormones subside
In prepubertal girls, large cysts can cause precocious puberty
In adolescents, ovarian cysts are very common
Usually due to dysfunctional ovulation
Cysts often spontaneously resolve
Large cysts take longer to resolve
Multicystic Dysplastic Kidney
More common in males
Left kidney more commonly affected
Distinguished from hydronephrosis as cysts do not connect with renal pelvis
Natural history is involution of kidney
Pancreatic Pseudocyst
Most common cystic lesion of pediatric pancreas
Can occur after blunt abdominal trauma or pancreatitis
Usually has thin, well-defined wall
Appendiceal Abscess
Seen after ruptured appendix
Occurs in ˜ 4% of appendicitis cases
More common in children < 4 years old
Patients have symptoms more than 3 days
Duplication Cyst
Can occur anywhere along GI tract
Located adjacent to GI wall
Usually spherical or tubular in shape
Lined with GI tract mucosa
Can have gastric mucosa in lining
Usually along mesenteric side
Ileum is most common site
Esophagus, duodenum next most common
Can create obstruction, bleeding, or intussusception
Helpful Clues for Less Common Diagnoses
Splenic Cyst
Can be congenital or acquired
Acquired cysts are due to trauma or infection
Congenital cysts are more common in girls
Has well-defined, thin walls
Calcifications can be seen within cyst wall
Urachal Cyst
Urachus remains patent between umbilicus and bladder
Can become infected
US shows thick-walled cyst above bladder
CT shows thick-walled cyst with surrounding inflammation
Hydrometrocolpos
Fluid-filled vagina + uterus
Can be caused by imperforate hymen, cervical stenosis, or atresia
Associated with anorectal malformations
Can lead to obstructive uropathy in neonate
Choledochal Cyst
Cystic or fusiform dilation of biliary tree
Todani classification with 5 types
Type 1 (cystic dilation of extrahepatic bile duct) is most common
Associated with ductal and vascular anomalies
Anomalous hepatic arteries, accessory ducts, and primary duct strictures
US is best screening test
HIDA scan can be used to prove connection to biliary system
Cystic Wilms Tumor
Most common abdominal neoplasm
Peak age is 3 years
Usually heterogeneous solid mass
Occasionally cystic mass
Helpful Clues for Rare Diagnoses
Meconium Pseudocyst
After meconium peritonitis
Underlying condition may be meconium ileus, volvulus, or atresia
Calcifications often present
On US, cyst is thick walled and echogenic
Multilocular Cystic Nephroma
a.k.a. multilocular cystic mass
Septae are only solid component
2 age peaks with differing pathology
Boys ages 3 months to 4 years: Cystic, partially differentiated nephroblastoma
Adult women: Cystic nephroma
Must be differentiated from cystic Wilms tumor
Mesenchymal Hamartoma
2nd most common benign hepatic tumor in children
85% present before age 3 years
Often presents as large RUQ mass
75% in right lobe of liver
α-fetoprotein can be elevated
Multiloculated cystic mass
Tiny cysts can appear solid
On US, septae of cysts can be mobile
Large portal vein branch may feed mass
Calcification is uncommon
Reports of malignant degeneration to undifferentiated embryonal sarcoma
Caroli Disease
a.k.a. type 5 choledochal cyst
May be associated with autosomal recessive polycystic kidney disease
Congenital cystic dilation of intrahepatic bile ducts
Presents with recurrent cholangitis or portal hypertension
Image Gallery
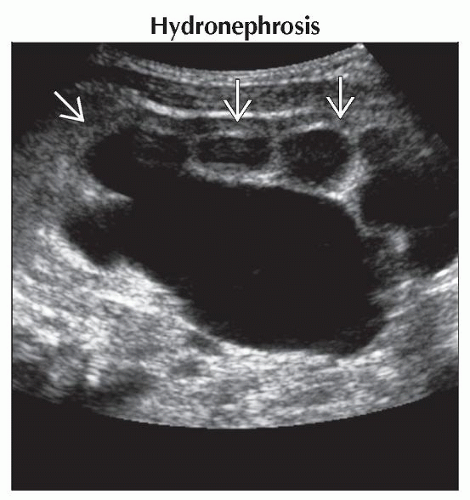 Longitudinal ultrasound shows marked hydronephrosis of the kidney  . Hydronephrosis is the most common abdominal mass in children and is most commonly caused by an obstruction of the ureteropelvic junction. . Hydronephrosis is the most common abdominal mass in children and is most commonly caused by an obstruction of the ureteropelvic junction. |
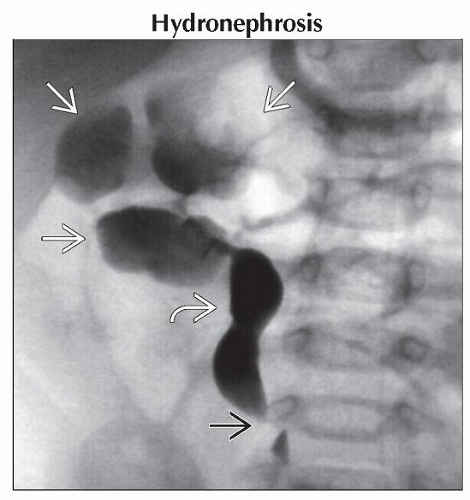 Anteroposterior retrograde pyelogram shows marked hydronephrosis with dilation of the renal calyces  . The ureter is dilated . The ureter is dilated  proximal to a focal area of narrowing near the ureteropelvic junction proximal to a focal area of narrowing near the ureteropelvic junction  . . |
 (Left) Transverse ultrasound in a 6-day-old girl shows an anechoic lesion
 arising from the ovary. There is a thin claw of normal ovarian tissue arising from the ovary. There is a thin claw of normal ovarian tissue  surrounding the cyst. Ovarian cysts are present in 98% of girls at birth due to maternal hormones. (Right) Axial CECT shows a large cystic mass surrounding the cyst. Ovarian cysts are present in 98% of girls at birth due to maternal hormones. (Right) Axial CECT shows a large cystic mass  extending from the pelvis to the mid-abdomen. The mass had simple characteristics on CT and ultrasound (not shown). Giant ovarian cysts such as this are uncommon. extending from the pelvis to the mid-abdomen. The mass had simple characteristics on CT and ultrasound (not shown). Giant ovarian cysts such as this are uncommon.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|