Cystic Abdominal Mass
Paula J. Woodward, MD
DIFFERENTIAL DIAGNOSIS
Common
Urinary Tract
Multicystic Dysplastic Kidney (MCDK)
Ureteropelvic Junction Obstruction
Enlarged Bladder
Urinoma
Gastrointestinal Tract
Bowel Atresia
Meconium Pseudocyst
Less Common
Ovarian Cyst
Lymphangioma
Enteric Duplication Cyst
Rare but Important
Choledochal Cyst
Neuroblastoma
Fetus-in-Fetu, Teratoma
Urachal Anomalies
Cloacal Malformation, Hydrocolpos
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Can the cystic mass be localized to a normal structure?
Most abdominal cystic masses are from the urinary tract
Gastrointestinal tract next most common
Is it a simple cyst or a complex cystic mass?
Septations, internal echogenic debris
What are the wall characteristics?
Thin-walled, thick-walled, calcified, “gut signature”
Is it constant or does it change appearance during the exam, between exams?
Helpful Clues for Common Diagnoses
Multicystic Dysplastic Kidney (MCDK)
Multiple cysts of varying sizes with no discernible renal parenchyma
Reniform shape is lost
Variable in utero course: May involute, remain stable, or grow
May be massive and cross midline
Ureteropelvic Junction Obstruction
May present as large cyst if severe obstruction
Look for communication with dilated calyces
Enlarged Bladder
Posterior urethral valves most common cause
Look for “keyhole” appearance created by the dilated posterior urethra
Prune belly syndrome and urethral atresia less common causes
Hydronephrosis also commonly seen
Urinoma
Spontaneous rupture of the renal collecting system into retroperitoneum
Look for contained fluid collection adjacent to obstructed kidney
Bowel Atresia
Can occur anywhere along gastrointestinal tract
Has a tubular, “sausage-shaped” appearance
Peristalsis within a cystic mass is pathognomonic
Meconium Pseudocyst
Wall-off bowel perforation
Irregular, thick walls
Look for other signs of meconium peritonitis
Intraperitoneal calcifications
Dilated bowel
Ascites
Helpful Clues for Less Common Diagnoses
Ovarian Cyst
Top consideration for a unilocular cyst in a 3rd trimester female fetus
“Daughter cyst” sign
Small cyst along wall of dominant cyst
Highly specific (up to 100%) sign for ovarian origin (82% sensitive)
May have occasional septations
If appearance becomes complex, with internal echoes, then there is concern for torsion
Occasionally found in upper abdomen
Supporting ligaments are lax, allowing for displacement
May occasionally be bilateral
Lymphangioma
Thin-walled cystic mass
May be unilocular or multilocular, with one or multiple septations
Can be very complex, insinuating around organs and extending out of abdomen
Variable echogenicity of fluid, but usually anechoic
Enteric Duplication Cyst
Solitary, thick-walled cyst
Look for “gut signature”
Layered appearance with echogenic mucosa, hypoechoic muscular layer, echogenic serosa
Often difficult to see in utero
Rarely bowel dilatation from obstruction
Helpful Clues for Rare Diagnoses
Choledochal Cyst
Cystic dilatation of extrahepatic &/or intrahepatic bile ducts
Unilocular, simple, right upper quadrant cyst is most common presentation in fetus
Round in axial plane and fusiform in longitudinal plane
Following bile ducts into cyst confirms diagnosis
Neuroblastoma
Arises from adrenal gland
Approximately 50% are cystic
Complex appearance with thick septations
Cystic neuroblastoma has an excellent prognosis
Fetus-in-Fetu, Teratoma
Overlapping features between these two entities
Fetus-in-fetu more developed and must have spinal elements
Complex, with a large solid component encapsulated within a cyst
Calcifications, including well-formed bones, most specific finding
Majority reported in upper retroperitoneum
Fetus-in-fetu theoretically result of inclusion of a monochorionic diamniotic twin within a host twin
Urachal Anomalies
Includes cysts and patent urachus
Communication with bladder confirms patent urachus
Bladder may appear elongated with a figure 8 or “waisted” configuration
May extend into base of umbilical cord
Associated with allantoic cord cysts
May resolve as gestation progresses
Cloacal Malformation, Hydrocolpos
Persistent cloaca
Failure of urorectal septum to reach perineum
Seen in female fetuses
Results in single perineal opening for urine, genital secretions, and meconium
Bladder, vagina, and rectum may all communicate in utero
Variable presentation
Cystic mass in pelvis
Dilated pelvic bowel loops; may see enteroliths from mixing of meconium and urine
Hydronephrosis and lumbosacral anomalies may also be present
Abnormal genitalia with lack of normal labial/clitoral formation
Ascites reported in some cases
Image Gallery
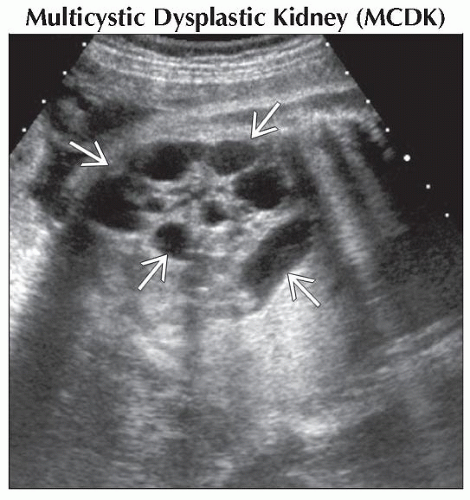 Coronal oblique ultrasound shows that the left kidney  is enlarged and cystic, consistent with a MCDK. Most abdominal cystic masses in the fetus are related to the urinary tract. is enlarged and cystic, consistent with a MCDK. Most abdominal cystic masses in the fetus are related to the urinary tract. |
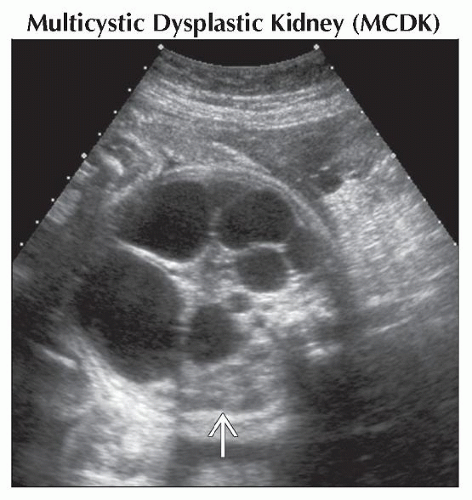 Axial ultrasound shows a cystic mass filling the fetal abdomen. When large, a MCDK can have a confusing appearance. Only one normal kidney  is seen, which is the key to the diagnosis. is seen, which is the key to the diagnosis. |
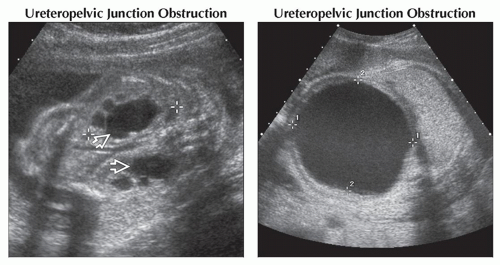 (Left) Coronal ultrasound shows classic bilateral ureteropelvic junction obstruction  in a 2nd trimester fetus. (Right) Axial ultrasound of the same fetus in the 3rd trimester shows dramatic progression, with massive left renal pelvis distention (calipers). When presenting late, this appearance may be confusing. Careful scanning may show dilated calyces. in a 2nd trimester fetus. (Right) Axial ultrasound of the same fetus in the 3rd trimester shows dramatic progression, with massive left renal pelvis distention (calipers). When presenting late, this appearance may be confusing. Careful scanning may show dilated calyces. |
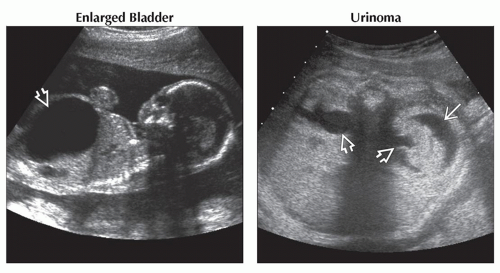 (Left) Sagittal oblique ultrasound shows marked distention of the bladder
 in this male fetus with posterior urethral valves. (Right) Axial ultrasound shows a fetus with bilateral UPJ obstruction in this male fetus with posterior urethral valves. (Right) Axial ultrasound shows a fetus with bilateral UPJ obstruction  . There was a unilateral collecting system rupture, partially decompressing the left collecting system. Urine is collecting in the perirenal space . There was a unilateral collecting system rupture, partially decompressing the left collecting system. Urine is collecting in the perirenal space  . Note how the fluid is surrounding and compressing the kidney, classic features of a urinoma. . Note how the fluid is surrounding and compressing the kidney, classic features of a urinoma.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|