Chapter 111 Contraception
Adolescents bear a disproportionate risk of the adverse consequences of sexual activity, sexually transmitted infections (STIs) (Chapter 114), and early, unintended pregnancy (Chapter 112). Adolescents often do not seek reproductive health care for 6 to 12 mo after initiating sex; many will become pregnant and/or acquire an STI during this interval. Youth who plan sexual initiation are 75% more likely to use contraception at sexual debut. Early adolescents are concrete thinkers, which may limit their ability to plan; most contraception requires some planning. Appropriate educational interventions with adolescents including the health care provider bringing up the topic of prevention can decrease sexual risk behavior.
Epidemiology
Sexual Activity
The median age at 1st intercourse varies greatly across the globe. Among participants ranging in age from 16 to above 65 yr representing all educational levels from 26 middle- and high-income nations, age of sexual debut was 18.9 yr for women and 19.5 yr for men, with an overall range of 23.0 yr in Malaysia to 17.3 yr in Austria (18.0 yr in the USA) (Fig. 111-1). Among developing nations, there is greater diversity; 73% of Liberian women ages 15-19 yr have had intercourse, compared to 53% of Nigerian, 49% of Ugandan, and 32% of Botswanan women. Only 7% of Chinese university students report being sexually experienced. Among U.S. high schools students in 2007, 7% report having initiated sex before age 13 yr, including 16% of African-American, 8% of Hispanic, and 4% of white youth; 48% of high school students are sexually experienced, including 67% African-American, 52% Hispanic, and 44% white.
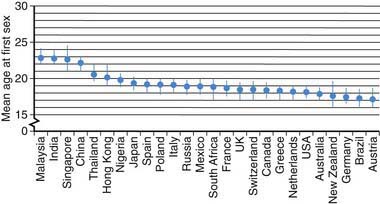
Figure 111-1 Mean age at first sex by country.
(From Durex Network: The face of global sex 2007. First sex: opportunity of a lifetime, Cambridge, UK, 2007, SSL International, p 13. www.durexnetwork.org/en-GB/research/faceofglobalsex/Pages/Home.aspx. Accessed April 22, 2010.)
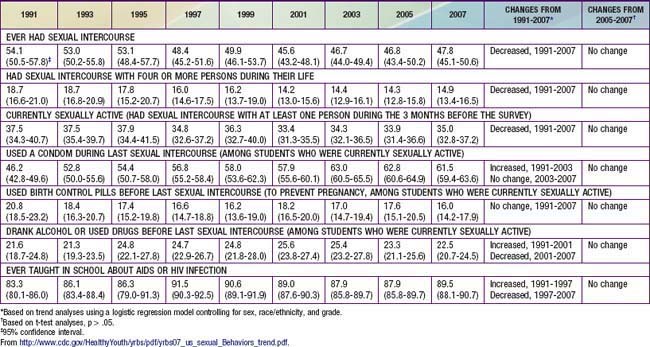
Despite decreases in adverse outcomes of adolescent sexual activity in the USA for the decade at the end of the 20th and beginning of the 21st century, this trend may be reversing. The annual rate of AIDS diagnoses reported among males aged 15-19 yr doubled in the past from 1.3 cases per 100,000 population in 1997 to 2.5 cases in 2006; and rates of gonorrhea and syphilis also increased. Birthrates among adolescents aged 15-19 yr decreased each year from 1991-2005 but increased from 40.5 live births per 1,000 females in 2005 to 42.5 in 2007. The USA has the highest rate of teen pregnancy in the western industrialized world. Of the >750,000 pregnancies among women aged 15-19 yr annually, ~ 80% are unintended (of which 30% are aborted). Consistent with these decreases and subsequent increases in adverse outcomes, the Centers for Disease Control and Prevention “Youth Risk Behavior Survey” reported that among high school students the rate of “ever had intercourse” declined from 54.1% in 1991 to 46.7% in 2005. From 2005 to 2007 there was no further decline; rather, albeit insignificant statistically, all 3 categories of sexual activity (ever had sex, number of partners, currently sexually active) showed increasing trends and both contraception reports (use a condom, use birth control) showed decreasing trends (Table 111-1).
Contraceptive Use
Use of contraception at first sex has increased over the past half-century. Among the residents of 26 middle- and high-income countries listed in Figure 111-2, individuals >65 yr were 8-fold more likely to have used no contraception for their sexual debut, compared to youth currently 16-19 yr of age (among whom 75% used contraception). Females compared to males were 25% more likely to use some form of contraception when they made their sexual debut. Factors increasing the use of contraception at sexual debut include: increasing age among teens up to age 17 yr; spending some time at college; and planning their sexual debut (75% more likely to have used contraception than those who did not plan it). Among U.S. men, data from the National Center for Health Statistics reveals that 48% of those 15-44 yr report using a condom the 1st time they had sex, while 71% of sexually experienced men age 15-19 yr report using a condom the 1st time they have sex. Use of a condom at last episode of intercourse increased from 46% in 1991 to 63% in 2003; in 2007 61.5% reported using a condom; use of birth control pills was 20.8% in 1991 and 16% in 2007 (see Table 111-1). Condoms were the most frequently used method, with dramatic increases from 1995-2002 in non-Hispanic white females (40.8% to 60.8%) and non-Hispanic black males (71% to 86.1%). The type of hormonal method selected also varies by ethnicity, with non-Hispanic white women more likely to select pills (40.7%); black women use pills as the first choice, and use the injectable method twice as much as white women.
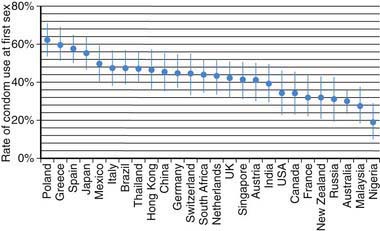
Figure 111-2 Rate of condom use at first sex by country.
(From Durex Network: The face of global sex 2007. First sex: opportunity of a lifetime, Cambridge, UK, 2007, SSL International. www.durexnetwork.org/en-GB/research/faceofglobalsex/Pages/Home.aspx. Accessed April 22, 2010.)
Contraceptive Counseling
The health screening interview during the adolescent preventive visit offers the opportunity both to support the adolescent who is abstinent to continue to be so and to identify the sexually active adolescent who has unsafe sexual practices (Chapter 106). Adolescents with chronic diseases are particularly vulnerable to having these issues omitted from the health maintenance visit (Chapter 39). There may be particular cautions related to concurrent medication to be noted for these chronically ill teenagers; sexuality and contraceptive issues do need to be addressed. The goals of a counseling intervention with the adolescent are to understand the adolescent’s perceptions and misperceptions about contraceptives, help him or her put the risk of unprotected intercourse in a personal perspective, and educate the adolescent regarding the real risk and contraindications for the various methods available.
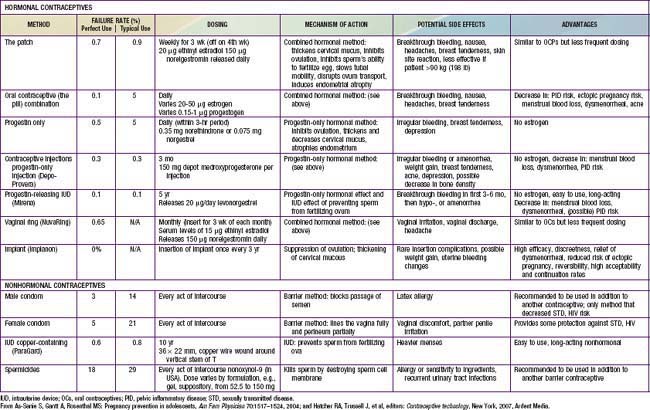
The likelihood that an adolescent will use a contraceptive method depends on such factors as the developmental level of the adolescent, the reproductive history, the involvement in other high-risk behaviors, and the degree of readiness for using contraception. Readiness to use contraception progresses in stages, from (1) precontemplative, not thinking about using contraception; (2) contemplative, giving it some thought, but having no immediate plans; (3) preparative, wanting to try a method in the near future; to (4) active, using contraception. The adolescent should also be made aware of the “perfect” use failure rates versus the “typical” failure rates based on the correct and consistent use of the method (Table 111-2). The pregnancy risk for use of withdrawal as a contraceptive method is probably underestimated in adolescents, and its low efficacy rate should be specifically addressed with young adolescents. Once an adolescent chooses a method, the provider and youth must discuss recognition of the common side effects, with clear plans on management; communication with the provider about the realistic expectation for failure; a contingency plan for that possibility; and strategies for close follow-up (see Table 111-2). A pelvic examination is not required for provision of a contraceptive method. Guidelines from the American College of Obstetrics and Gynecology stipulate that a routine pelvic exam with Pap smear be initiated 3 yr after onset of sexual activity. After this event, annual urine screening for STIs is advised. Confidentiality and consent issues related to contraceptive management are discussed in Chapter 106.
111.1 Barrier Methods
Condoms
This method prevents sperm from being deposited in the vagina. There are no major side effects associated with the use of a condom. The risk of AIDS may have increased the use of condoms among adolescents, with 46.2% of high school students in 1991 reporting using a condom at last sexual intercourse increasing to 61.5% in 2007. Condom use rates vary considerably between countries; condom use at 1st intercourse is higher in many countries compared to the USA (see Fig. 111-2). The main advantages of condoms are their low price, availability without prescription, little need for advance planning, and, most important for this age group, their effectiveness in preventing transmission of STIs, including HIV and human papillomavirus (HPV). Latex condoms are recommended as protection against STIs, to be used along with all nonbarrier medical methods for adolescents. A female condom is available over the counter in single size disposable units. It is a 2nd choice over the male latex condom because of the complexity of properly using the device, its low typical efficacy rate, and the lack of studies in humans demonstrating its effectiveness against STIs. Most adolescents would require intensive education and hands-on practice to use it effectively.



