Congenital Malformations
Lewis B. Holmes
FREQUENCY OF MAJOR AND MINOR ANOMALIES
A major malformation is usually defined as a structural abnormality that has surgical, medical, or cosmetic importance. Major malformations are more common in spontaneously aborted fetuses than in term infants. Approximately 2% of infants of at least 20 weeks’ gestational age have a major malformation (Table 19.1). The frequency of malformations is higher among older children, because hidden abnormalities, such as kidney malformations and mild heart defects, have been detected. Having a single major malformation is much more common than having multiple malformations.
Minor anomalies are much more common than major malformations. A minor malformation is an abnormality that has no surgical or cosmetic significance (Fig. 19.1). These malformations occur in fewer than 4% of all newborns of the same race and gender. Minor physical features that occur in more than 4% of infants are considered normal variations. The frequencies of specific minor physical features vary among racial groups. For example, preauricular sinus and accessory nipples are more common among black than among white infants (Table 19.2). The pediatrician examining newborn infants should expect to find a few minor anomalies and normal variations. Finding three or more minor anomalies should prompt a careful assessment for the presence of a major malformation, because they are present in approximately 20% of these infants. Finding some specific minor anomalies may necessitate further diagnostic study. For example, an infant found to have a branchial sinus and a preauricular tag or sinus may have the branchio-oto-renal syndrome, a hereditary disorder in which serious kidney malformations occur. A capillary hemangioma and lipoma over the lumbar spine can be a sign of a lipomeningocele, in which tethering of the spinal cord can occur.
RECOGNIZED ETIOLOGIES OF MALFORMATIONS
The causes are known for about 60% of major malformations. Chromosome abnormalities include trisomy, deletion, unbalanced translocations, and uniparental disomy. Deletions should be tested for with fluorescent in situ hybridization (FISH) techniques for special malformations, such as chromosome 22q11.2 deletion in infants with heart defects and chromosome 17p13.3 deletion in infants witth lissencephaly. Subtelomeric deletion studies identify subtle chromosome deletions in about 5% of children with anomalies and developmental delay. Thousands of malformations attributed to autosomal dominant, autosomal recessive, and X-linked etiologies have been cataloged and are usually diagnosed by clinical comparisons (http://www-ncbi-nlm-nih-gov.easyaccess1.lib.cuhk.edu.hk/omim/). Molecular testing may be available to confirm the diagnosis. The laboratories providing molecular testing for specific malformations can be identified from GeneTests (http://www.genetests.org).
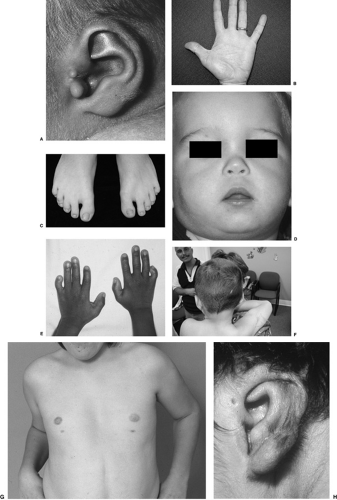 FIGURE 19.1. Examples of minor anomalies. A: Preauricular tag. B: Simian crease, left hand. C: Syndactyly, toes 2 to 3. D: Anteverted nostrils. E: Bilateral clinodactyly, finger 5. F: Double hair whorl G: Bilateral extra nipple. H: Preauricular sinus. (All photos courtesy of the Greenwood Genetic Center, Greenwood, South Carolina.) |
Malformations Caused by Multifactorial Inheritance
The most common malformations (e.g., heart defects and spina bifida) are attributed to multifactorial inheritance, a process in which mutant genes and environmental factors are presumably involved. For all malformations attributed to multifactorial inheritance, the likelihood that a subsequent sibling (or the offspring of an affected parent) will be affected is 10 to 20 times greater than the risk in the general population (Table 19.3) but less than in instances involving autosomal recessive and autosomal dominant genes with complete penetrance. As an example of an environmental factor, periconceptional supplementation with folic acid decreases significantly the occurrence of anencephaly or spina bifida and heart defects. Several genetic abnormalities have been identified that are associated with the occurrence of spina bifida as well as Hirschsprung disease. Some studies have shown a strong interrelationship between maternal cigarette smoking, the presence of specific genetic markers, and the occurrence of either orofacial clefts or low birth weight.
TABLE 19.1. CONGENITAL MALFORMATIONS IN NEWBORN INFANTS: RECOGNIZED ETIOLOGIES* | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


