Congenital Aortic Anomalies
Eric J. Crotty, MD
DIFFERENTIAL DIAGNOSIS
Common
Left Aortic Arch with Aberrant Right Subclavian Artery
Aortic Coarctation
Double Aortic Arch
Less Common
Right Aortic Arch with Aberrant Left Subclavian Artery
Right Aortic Arch with Mirror-Image Branching
Rare but Important
Interrupted Aortic Arch
Cervical Aortic Arch
Persistent 5th Aortic Arch
Pulmonary Sling
ESSENTIAL INFORMATION
Helpful Clues for Common Diagnoses
Left Aortic Arch with Aberrant Right Subclavian Artery
Right subclavian artery has separate origin as last vessel from arch or proximal descending aorta
No diverticulum at origin of aberrant right subclavian artery
Patients usually asymptomatic as no vascular ring is present
Radiograph may show left aortic arch and impression on posterior wall of trachea
Esophagram, AP view
Impression on left side of barium column, which continues obliquely superiorly and to right
Esophagram, lateral view
Posterior indentation on barium column on lateral view
CT and MR will show aberrant right subclavian artery coursing posterior to esophagus and superiorly to right
Aortic Coarctation
Focal narrowing of upper thoracic aorta at level of insertion of ductus arteriosus
Less commonly long segment or may be associated with diffuse tubular hypoplasia of aortic arch and isthmus
Cardiomegaly and increased pulmonary vascularity with edema may be present in infants
“3” sign may be present
Notching of undersurface of ribs may develop in longstanding severe cases
Collateral flow best identified by CTA and MRA; can be quantified by MR
Double Aortic Arch
Both limbs usually complete, but 1 side may be atretic (30%)
Atretic limb remains in fibrous continuity with descending aorta
Although variable, right limb is usually larger (dominant) and higher in position than left
Most commonly: Left arch anterior and left of trachea, right arch posterior and right of esophagus
Limbs join posteriorly to form left-sided descending aorta
Symptoms usually present early
Radiograph may show dominant arch and compression on both sides of trachea
Esophagram, AP view
Compression on both sides of esophagus
Esophagram, lateral view
Posterior impression
CT and MR demonstrate relative sizes of limbs and degree of associated tracheal narrowing
Rarely associated with intracardiac defects
Helpful Clues for Less Common Diagnoses
Right Aortic Arch and Aberrant Left Subclavian Artery
Left subclavian artery has separate origin
Last vessel from arch or proximal descending aorta
May be associated with diverticulum of Kommerell
Radiograph may show right aortic arch and impression on posterior wall of trachea
Esophagram, AP view
Impression on right side of barium column which continues obliquely superiorly to left
Esophagram, lateral view
Posterior indentation on esophagus
CT and MR will show aberrant left subclavian artery coursing posterior to esophagus and superiorly to left
Vascular ring completed by left ligamentum arteriosum to left pulmonary artery
Low association (10%) with intracardiac defects
Right Aortic Arch with Mirror-Image Branching
3 vessels arise from right aortic arch in following order
Left innominate artery coursing anterior to trachea
Right carotid artery
Right subclavian artery
Impression on right side of trachea and right arch are visible on frontal chest radiograph
Lateral chest radiograph does not show impression on posterior wall of trachea
Esophagram, AP view
Shows corresponding impression on right wall of esophagus
Esophagram, lateral view
No impression on posterior wall of esophagus
High association (90%) with intracardiac defects
Tetralogy of Fallot, truncus arteriosus, and double-outlet right ventricle most common defects
Helpful Clues for Rare Diagnoses
Interrupted Aortic Arch
Interruption may occur at different sites along arch
Most common site is between origins of left carotid artery and left subclavian artery (2/3 of cases)
Postnatally, blood supply to lower half of body requires patent ductus arteriosus
Cervical Aortic Arch
Arch found above level of clavicle
May reach level of C2 vertebra
Usually right arch
May have associated symptomatic vascular ring
Persistent 5th Aortic Arch
Both arches appear on same side of trachea with superior-inferior relationship
Both arches may be patent or superior arch may be interrupted with patent inferior arch
Pulmonary Sling
Origin of left pulmonary artery has distal origin from main pulmonary artery and courses sharply to left
Passes between trachea and esophagus
Associated with long-segment tracheal narrowing
Narrowing due to complete tracheal rings and anomalous tracheal branching
Image Gallery
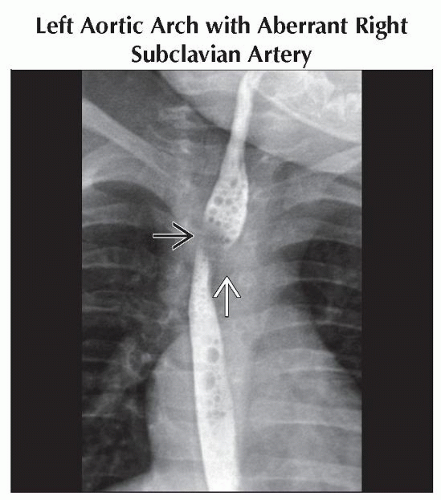 Anteroposterior esophagram shows a left aortic arch displacing the esophagus to the right  . There is a filling defect in the contrast column running obliquely and superiorly to the right . There is a filling defect in the contrast column running obliquely and superiorly to the right  . . |
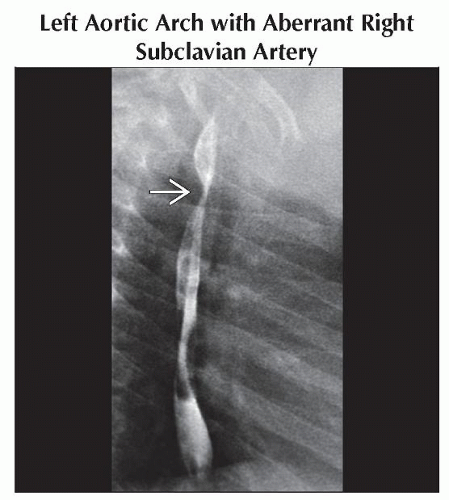 Lateral esophagram shows a posterior impression on the esophagus  . The findings on the AP and lateral views are consistent with a left aortic arch with an aberrant right subclavian artery. . The findings on the AP and lateral views are consistent with a left aortic arch with an aberrant right subclavian artery. |
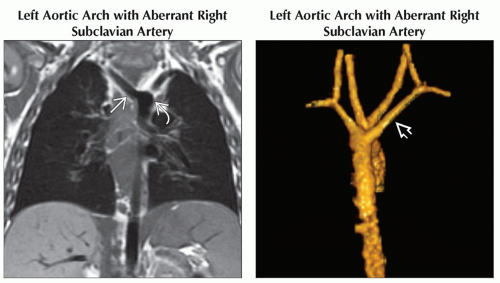 (Left) Coronal T1WI MR shows a left-sided aortic arch  with an aberrant right subclavian artery with an aberrant right subclavian artery  . Because the ligamentum arteriosum is on the left side, there is no vascular ring, and the patients are often asymptomatic. Pressure on the esophagus may cause dysphagia. (Right) Posterior 3D reconstruction shows the aberrant subclavian artery . Because the ligamentum arteriosum is on the left side, there is no vascular ring, and the patients are often asymptomatic. Pressure on the esophagus may cause dysphagia. (Right) Posterior 3D reconstruction shows the aberrant subclavian artery  as the last vessel from the arch. CT and MR are replacing UGI studies for investigating vascular rings. as the last vessel from the arch. CT and MR are replacing UGI studies for investigating vascular rings. |
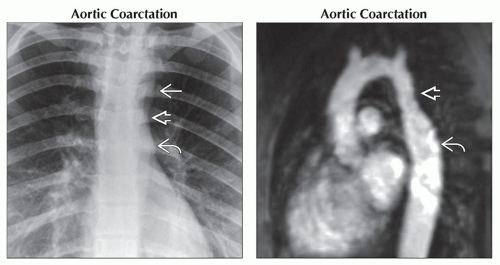 (Left) PA radiograph shows the “3” sign. A superior convexity
 of the aortic arch is followed by the concavity of the coarctation of the aortic arch is followed by the concavity of the coarctation  and a lower convexity caused by poststenotic dilatation and a lower convexity caused by poststenotic dilatation  . Most coarctations are corrected before radiographic signs have time to develop. (Right) Oblique MRA in the same patient shows the coarctation . Most coarctations are corrected before radiographic signs have time to develop. (Right) Oblique MRA in the same patient shows the coarctation  with poststenotic dilatation with poststenotic dilatation  of the proximal descending aorta. of the proximal descending aorta.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|