
To Aid Other Diagnostic Tests
Amniocentesis and chorionic villus sampling (CVS) are performed under ultrasound vision.
As a Diagnostic Test
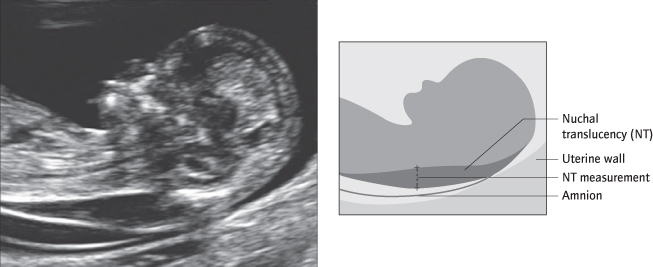
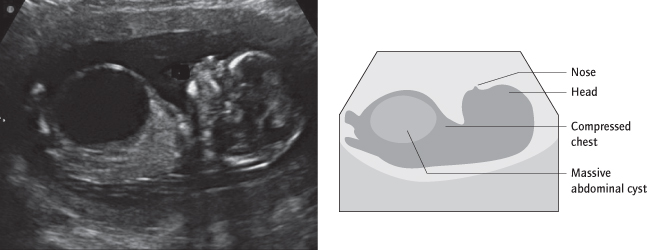
Structural abnormalities are usually diagnosed at 18–21 weeks at the ‘anomaly scan’. Congenital malformations of all organs and systems are detectable. At least 25% of abnormalities can actually be identified at 11–14 weeks at the time of nuchal translucency assessment (Fig. 18.4). However, particularly with the heart, many remain undiagnosed even at 20 weeks, and this is related to operator experience. In addition, some abnormalities do not become evident until later either because they are not visible or because they develop with gestation. The development of increased liquor volume, polyhydramnios [→ p.164], in later pregnancy can be the result of a fetal abnormality and warrants a repeat detailed ultrasound examination.
Fetal Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) scanning of the fetus in utero is increasingly used in the diagnosis of intracrania lesions and is better at differentiating between different types of soft tissue, e.g. liver and lung. It may also have a role as an alternative to postmortem examination.
3-D/4-D Ultrasound
3-D or real time 3-D (known as 4-D ultrasound) using a computer reconstructed 3-D ultrasound image can allow better evaluation of certain abnormalities, and is being intensively used, largely in tertiary referral centres.
Amniocentesis
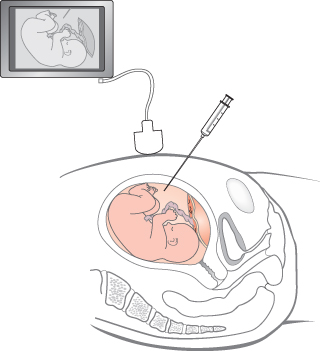
This is a diagnostic test, involving removal of amniotic fluid using a fine-gauge needle under ultrasound guidance (Fig. 18.5). It is safest performed from 15 weeks’ gestation, and it may be done later. This enables prenatal diagnosis of chromosomal abnormalities, some infections such as cytomegalovirus (CMV) and toxoplasmosis, and inherited disorders such as sickle-cell anaemia, thalassaemia and cystic fibrosis. One per cent of women miscarry after an amniocentesis (Obstet Gynecol 2006; 108: 1067).
Chorionic Villus Sampling
This diagnostic test involves biopsy of the trophoblast, by passing a fine-gauge needle through the abdominal wall or cervix and into the placenta, after 11 weeks: the result is therefore obtained faster than with amniocentesis and allows an abnormal fetus to be identified at a time when abortion, if requested, could be performed under general anaesthesia. The miscarriage rate is slightly higher than after amniocentesis, but this is because it is performed earlier, when spontaneous miscarriage is more common, and because it is a more difficult procedure. It is used to diagnose chromosomal problems and autosomal dominant and recessive conditions.
With both amniocentesis and CVS, fluorescence in situ hybridization (FISH) and polymerase chain reaction (PCR) can both be used to diagnose the most common abnormalities in less than 48 h.
Preimplantation Genetic Diagnosis
In vitro fertilization (IVF) allows cell(s) from a developing embryo to be removed for genetic analysis before the embryo is transferred to the uterus. This allows selection, and therefore implantation, only of embryos that will not be affected by the disorder for which it is being tested. The technique is expensive and presents ethical dilemmas, but has been used in prenatal diagnosis of sex-linked disorders, trisomies, and both autosomal dominant and recessive conditions. It does require IVF, even in couples who are fertile.
Chromosomal Abnormalities
These affect 6 per 1000 live births, but are much more common in early pregnancy as a cause of miscarriage. Most are trisomies.
Down’s Syndrome
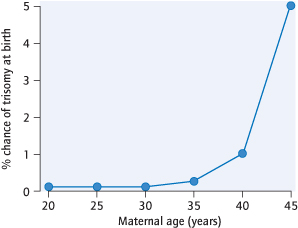
Trisomy 21 is the most common chromosomal abnormality among live births. It is usually the result of random non-dysjunction at meiosis, although occasionally (6%) it arises as a result of a balanced chromosomal translocation in the parents. It is more common with advancing maternal age (Fig. 18.6). The affected infant has mental retardation, characteristic facies and often (50%) congenital cardiac disease. Other structural abnormalities may also be present. Unless the result of a parental balanced translocation, the recurrence risk is low and determined largely by maternal age.
The Nuchal Scan
Ultrasound component of ‘combined test’ for aneuploidy
Dates pregnancy, determines chorionicity in multiples
Many structural abnormalities visible
Other Chromosomal Abnormalities
Trisomy 18 (Edward’s syndrome) and trisomy 13 (Patau’s syndrome) are also more common with advanced maternal age. They are associated with major structural defects, and affected fetuses die in utero or shortly after birth. Sex chromosome abnormalities include Klinefelter’s syndrome (47 XXY). These males have normal intellect, small testes and are infertile. In Turner’s syndrome (a single X chromosome only: X0), affected individuals are female, infertile but with normal intellect.
Risk Factors for Down’s Syndrome
| History: | High maternal age |
| Previous affected baby (risk increased 1%) | |
| Balanced parental translocation (rare) | |
| Ultrasound: | Thickened nuchal translucency |
| Some structural abnormalities | |
| Absent or shortened nasal bone | |
| Triscuspid regurgitation | |
| Blood tests: | Low pregnancy-associated plasma protein A (PAPP-A) (1st trimester) |
| High human chorionic gonadotrophin beta-subunit (β-hCG) (1st/2nd trimester) | |
| Low alpha fetoprotein (AFP) (1st/ 2nd trimester) | |
| Low oestriol (2nd trimester) | |
| High inhibin (2nd trimester) |
Screening and Diagnosis of Chromosomal Abnormalities
Amniocentesis and CVS are diagnostic tests for chromosomal abnormalities. Traditionally they have been offered to women over the age of about 35 years. However, younger women have more babies and therefore, despite a lower individual risk, account for more Down’s syndrome pregnancies. These would go undetected without a screening programme for all consenting women.
In the UK, the National Screening Committee (www.nsc.nhs.uk) recommends that all pregnant women are offered a screening test for trisomies including Down’s syndrome, which for the latter has a 75% sensitivity and for a 3% false positive rate. This can be achieved by integrating the risk from maternal age, with PAPP-A and β-hCG blood tests, and nuchal translucency measurement by ultrasound at 11–13 + 6 weeks in what is called the ‘combined test’. The ‘triple test’, a blood test at 16 weeks which uses AFP, hCG and oestriol, is less accurate and does not meet these standards. It should be reserved for where screening is performed later than 14 weeks. It nevertheless remains in use where nuchal translucency scanning is not available because, not requiring a detailed ultrasound scan, it is less expensive.
A bewildering array of screening tests exist. These broadly are divided into three types; intimate knowledge of these is not required:
1 The risk at a nuchal translucency scan can be modified by other risk factors at this scan: markers include the presence or absence of the nasal bone (Lancet 2001; 358: 1665), and tricuspid regurgitation (Ultrasound Obstet Gynecol 2005; 26: 22). Less widely accepted and requiring considerable expertise, they may lead to better detection rates in the future.
2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


