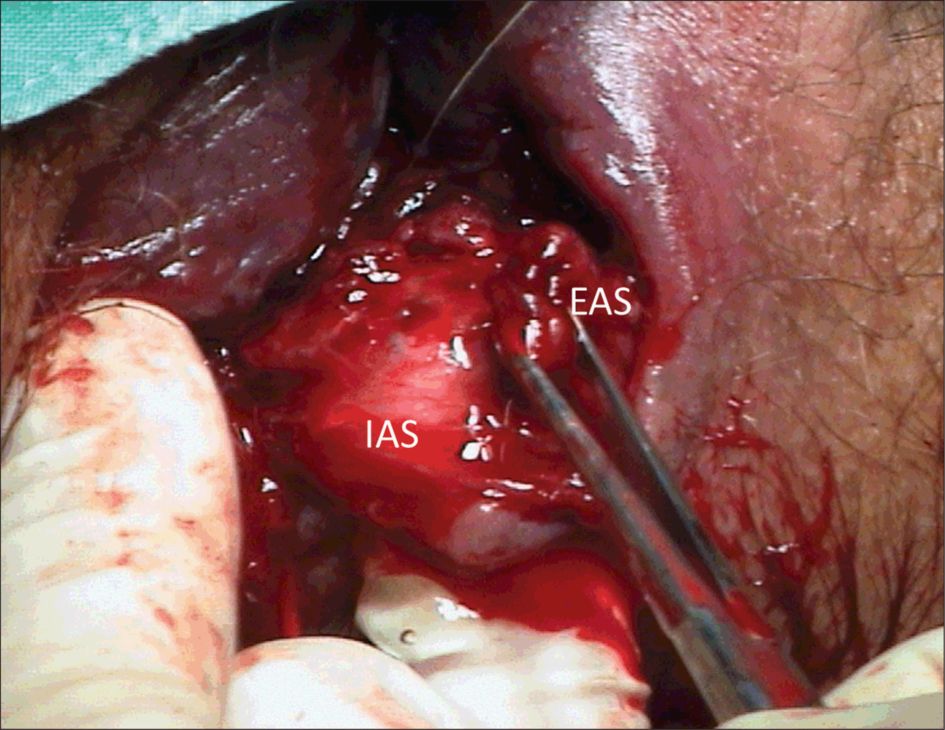
Third degree tear (Grade 3b) with the external AS (EAS) grasped by Allis forceps, the ischioanal fat is lateral to the EAS
It is essential that, prior to examination or suturing, the procedure is explained to the woman and her partner and consent obtained.
Repair of perineal trauma
1 Excessive uterine bleeding should be managed appropriately prior to commencing the perineal suturing.
2 Ensure that the wound is adequately anaesthetised prior to commencing the repair
a) local infiltration with 1% lignocaine is adequate for simple trauma, but extensive damage and difficult repairs may need more effective analgesia than the maximum dose of 20ml will achieve. Always be careful to avoid injecting directly into a vessel.
b) top up an existing epidural or administer regional anaesthesia; this is especially worthwhile for extensive trauma where access is difficult (e.g. high fornices trauma), or where the anal sphincter complex is involved.
3 A quick assessment should be made as to whether the operator is capable of completing the repair, as this facilitates request for senior assistance rather than struggling for ages before admitting defeat, during which time significant blood loss may have occurred.
Current research suggests that perineal trauma should be repaired using the continuous non-locking technique to reapproximate all layers in turn (vagina, perineal muscles and then subcuticular to the skin) with absorbable polyglactin 910 material (Vicryl rapide®).
Be careful to identify the apex and check the extent of the trauma; whether the trauma is unilateral or bilateral and how deep it goes. The first stitch is inserted 5–10 mm above the apex of vaginal trauma to secure any bleeding points that may not be visible, and thence proceeds caudally. Any large bleeding vessels should be secured individually rather than ‘hiding them’ as continued bleeding can occur, concealed from view, to produce an ischiorectal haematoma.
Check that the finished repair is anatomically correct, and complete haemostasis is achieved. Perform a vaginal examination, and check that the vagina is not stitched too tight.
A rectal examination should be performed after completing the repair to ensure that suture material has not been accidentally inserted through the rectal mucosa.
Check that all swabs, needles and instruments are correct.
Following completion of the repair, the extent of the injury sustained, the suture technique and materials used must be documented in the case notes in black ink. It is also useful to include a diagram to illustrate the extent of the trauma.
Repair of third and fourth degree tears
1 A repair should be performed only by a doctor experienced in anal sphincter repair or by a trainee under supervision. If in any doubt about diagnosis, it would be prudent to inform the consultant and await a second opinion (see DVD – www.perineum.net).
2 Colorectal surgeons are not needed for straightforward third and fourth degree tears but the height of the damage when the tear is fourth degree is vital to assess; if the tear extends beyond the anal canal into the rectum above the levator plate then a defunctioning colostomy may be indicated and a surgical colleague should be involved (tears of this severity are rare).
3 Third and fourth degree tears should usually be repaired in the operating theatre where there is access to good lighting, appropriate equipment and aseptic conditions. The perineal repair pack should contain appropriate instruments (demonstrated in Figures 36.3 and 36.4).
4 General or regional (spinal/epidural) anaesthesia is an important pre-requisite, particularly for overlap repair, as the inherent tone of the sphincter muscle can cause the torn muscle ends to retract within the sheath. Muscle relaxation is necessary to retrieve the ends, especially if it is intended to overlap the muscles without tension.
5 The full extent of the injury should be evaluated by a careful vaginal and rectal examination in lithotomy, and graded according to the classification above.
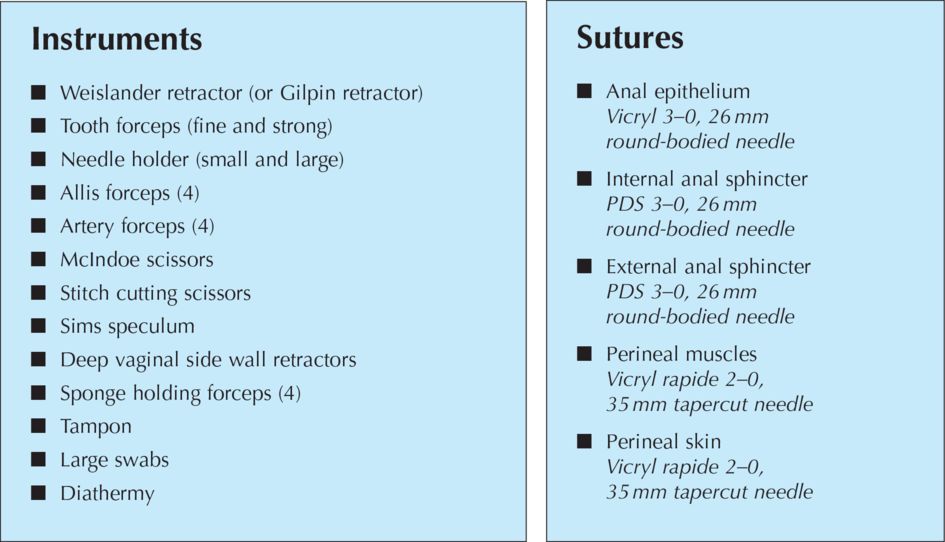
Instruments and sutures used for repair of AS trauma

Step 1: suturing the anal epithelium
In the presence of a fourth-degree tear, the torn anal epithelium is repaired with polyglactin 3/0 (Vicryl®, Ethicon, Edinburgh, UK). Continuous or Interrupted sutures can be used ( knots tied in the anal lumen).
Step 2: suturing the anal sphincter
(Prior to repairing the anal sphincter it is often worth securing the apex of the vaginal tear while access to it is facilitated by the sphincter tear, and then leave the suture with its needle protected ready to be completed later).
When torn the internal anal sphincter (IAS) should be identified and sutured separately from the external anal sphincter (EAS). The internal anal sphincter lies between the external sphincter and the anal epithelium. It is paler (raw fish-like) than the striated external sphincter (red meat-like) (Figure 36.5) and the muscle fibres run in a longitudinal fashion rather than the circular external sphincter. A torn internal sphincter should be approximated (not overlapped) with interrupted or mattress sutures using a fine monofilament suture material such as 3–0 polydiaxanone (PDS) or braided 2–0 polyglactin (Vicryl). It is very important for obstetricians to identify and repair the torn internal sphincter as colorectal surgeons find it almost impossible to identify and therefore repair as a secondary procedure if these women present with faecal incontinence.