Complementary and alternative medicine (CAM) has come into common use with as many as 40% of adult Americans and up to 12% of children have used CAM in the last 12 months, and in the year prior to a 2007 survey, Americans spent $33.9 billion out of pocket, accounting for 11.2% of total out-of-pocket health care expenditures for the year.1 The use of CAM side by side with conventional medicine is known as integrative medicine—the practice of medicine with the central focus on the physician-patient relationship and where healing, not curing, is the goal of therapy. Integrative medicine involves both conventional and complementary methods, first attempting natural and less invasive interventions before moving to more costly and invasive interventions while incorporating the patient’s mind, body, spirit, and community in healing. Sometimes, the term “holistic medicine” is used to describe this type of practice.2
Offering advice to graduating medical students in 1889, Sir William Osler stated that putting the patient’s interests first is the key to practicing medicine well. He stressed also the importance of physician self-care.3 When the focus of a medical encounter is on the whole patient, not on the mode of practice or the doctor, a truly healing relationship becomes possible. In such a relationship, the patient is central and his or her doctor acts as a guide, advisor, or consultant.
Critics of conventional allopathic medicine argue that in its attempts to be more scientific, Western medicine “underestimates the individuality of patients and pigeonhole[s] (sic) them within a clinical pseudo-democracy.”4 This approach values typology, not variation and individuality. In trying to understand why the use of CAM is increasing, Xu and Chen5 noted: “… biomedicine is at its limits nowadays when confronting degenerative diseases, stress-related diseases, and most chronic diseases, which are more related to the way we think and live than to bacteria and viruses. Most notably, biomedicine lacks reference to the self-healing capacity of the human mind and body and focuses on parts rather than the whole, treatment rather than prevention, the suffering disease rather than the diseased person.”
Patients, like all human beings, want to be considered and treated as the individuals they are, and with the context of their lives, including their beliefs, histories, and experiences taken into account. Patients want a therapeutic approach to be based on both evidence as well as the idea that what differentiates each of us as individuals is central to our health and to healing. Healing is the work of the body, and the fundamental role of medicine is to help the body do this.
Providers should give their patients their undivided attention while they tell their story because there is an element of healing that comes with being truly heard. Authentic listening, the combination of active listening as well as reflecting back through a reconstruction of what the patient is thinking and feeling, provides a way for clinicians to help connect with patients, as well as their colleagues and even themselves at a myriad of levels.6 Sometimes, in the simple act of telling of her story, a patient can begin to make connections and increase her understanding of her own situation. When the story is reflected back and clarifications or corrections are sought, the patient is reminded that they control the story, which often increases her insight(s) as well as the clinician’s.
In 1948, the World Health Organization (WHO) defined health as “a state of complete physical, mental and social well-being and not merely the absence of disease and infirmity.”7 Physicians focus rightly on the biomedical well-being of patients, but this is not enough. Curing patients is a rarity and is not always possible. By focusing on the whole patient, listening to her story, understanding her social situation, and encouraging her to be an active partner in her health, providers can bring about healing.
The WHO definition notes that traditional medicine refers to the knowledge, skills, and practices based on the theories, beliefs, and experiences indigenous to different cultures, used in the maintenance of health and in the prevention, diagnosis, improvement, or treatment of physical and mental illnesses.8 In 1992, the U.S. National Institutes of Health (NIH) Office of Alternative Medicine was established. The office was later upgraded to the National Center for Complementary and Alternative Medicine (NCCAM). In contrast to the WHO view of traditional medicine, NCCAM views CAM as “a group of diverse medical and health care interventions, practices, products, or disciplines that are not generally considered part of conventional medicine” and freely admits the boundaries between CAM and conventional medicine are not absolute.9
The mission of NCCAM is “to define, through rigorous scientific investigation, the usefulness and safety of complementary and alternative medicine interventions and their roles in improving health and health care.”10 The three long-range goals of NCCAM are to advance the science and practice of symptom management; develop effective, practical, personalized strategies for promoting health and well-being; and help create and facilitate the creation of evidence used in decisions around CAM and its integration into health care and health promotion. There are five major objectives for NCCAM:
Advance research on mind and body interventions, practices, and disciplines.
Advance research on CAM natural products.
Increase understanding of “real world” patterns and outcomes of CAM use and its integration into health care and health promotion.
Improve the capacity of the field to carry out rigorous research.
Develop and disseminate objective, evidence-based information on CAM interventions.
Common categories of CAM include natural products (e.g., herbs, supplements, probiotics), mind and body medicine (e.g., tai chi), manipulative and body-based practices such as massage therapy, movement therapies such as Pilates, traditional healing or indigenous practices, energy therapy, and whole medical systems such as Ayurvedic or traditional Chinese medicine.
Western medicine, or allopathic medicine, is one system of health care. But there are other nonallopathic systems of health care and, like allopathic medicine, they also seek to improve health and well-being for patients, families, communities, and society. In many countries in Europe, naturopathic medicine is a mainstream approach and includes nutrition, exercise, hydrotherapy, and other forms of physical therapy. All medical systems are embedded in their cultures. As a result, certain aspects of a medical system believed to be meaningful to one group may be meaningless to another group in another cultural setting. When confronted with a new idea, a common reaction is to “translate” the idea into familiar terms or concepts. A key issue that is often overlooked is that “identical” or “translatable” terms often have different meanings in the context of different medical systems.
Medical pluralism is a term used to describe the existence of separate medical systems within a single society. The integrative medicine model seeks to integrate conventional, allopathic medicine with CAM modalities that have demonstrated strong scientific evidence of safety and effectiveness. In the efforts to create a more integrated model, however, critics note that under the guise of altruism and an interest in public safety, efforts are made to ensure that alternative practitioners are regulated, educated, and professionalized in a fashion similar to biomedical practitioners. This may constrain CAM’s ability “to challenge, resist, and transform the hegemony and inequalities of biomedicine.”11
This chapter provided a brief overview of several other systems of health care and various CAM modalities. In addition, there is a brief review of some of the CAM modalities used for common office gynecology concerns.
ASSESSING THE RISKS AND BENEFITS OF COMPLEMENTARY AND CONVENTIONAL THERAPIES
Navigating the worlds of conventional medicine and alternative therapies can be complicated. Many patients, including pregnant women, believe that natural remedies are safer and more effective than chemical drugs prescribed by doctors and they do not view the use of herbs or supplements as being chemical in nature.11,12 Many patients do not disclose their use of CAM for fear of a negative response, the belief that clinicians do not need to know about it, or simply because they are not asked about it.13 The problem is that some CAM treatments do have potential for risks and harm and may interact adversely with conventional pharmacologic therapies. These interactions may occur through a reduction in effectiveness of prescribed treatments or they may interact with the CYP cytochrome P450 enzymes in the liver that impact drug metabolism, particularly the CYP cytochrome P450 3A4 isoform (referred to as CYP3A4). Some herbs and supplements may accelerate or slow the action of these enzymes and thus impact the functional dose of a drug the patient is concurrently using.
One recent study showed that among 200 women receiving chemotherapy for ovarian cancer, 40% were using one or more CAM supplements that might interact poorly with their chemotherapy regimen and many patients took multiple supplements.14 Only 42% discussed the use of CAM supplements with the conventional provider and even fewer 24% consulted with a CAM provider about the supplements they used. The study did not find that women were necessarily having ill effects from their use of CAM, but it does highlight that there is a high risk for ill effects and that further research in the use of ingestible CAM therapies with conventional medical therapies is needed.
One of the criticisms of CAM is that it lacks clinical trials and is not “evidence based”; however, this is not necessarily true. There are many peer-reviewed journals reporting on clinical trials, as well as many basic research endeavors into understanding and evaluating the mechanisms of action, safety, and efficacy of various CAM approaches. It is also critical to recall that because nonallopathic systems of health and medical care use very different theoretical frameworks, it is extremely difficult, if not impossible in some instances, to use conventional research methodology where participants are selected by standard diagnostic criteria that are not easily applicable in alternative systems of care.
Patients will use and even ask about CAM therapies and they want their clinicians to be able to provide balanced, nonjudgmental recommendations. The Institute of Medicine recommends that health professional schools incorporate information about CAM into curricula at the undergraduate, graduate, and postgraduate levels.15 Curriculum guidelines for integrative medicine have been published for medical students as well as residents, and some training programs have successfully created integrative medicine residency programs.16,17 Currently, there are over 40 academic Integrative Medicine centers (go to Consortium of Academic Health Centers for Integrative Medicine at http://www.ahc.umn.edu/cahcim) conducting high-quality research and using the practice of integrative health care at their institutions.
It is not possible for a clinician to keep up with the burgeoning amount of evidence in conventional medicine and nonconventional medicine or nonallopathic health care systems. However, conventional practitioners do need to ask their patients about their use of CAM, be familiar with the various modalities, know what credible resources exist to refer patients to, and to develop relationships with accredited local and regional programs and practitioners that offer integrative or CAM approaches (Table 20.1).
INTEGRATIVE MEDICINE MODALITIES
Lifestyle
Lifestyle encompasses eating and exercise habits as well as how people cope with stress and relate to families and friends. Many patients would benefit from lifestyle modification that involves increasing physical activity and decreasing food intake. Helping patients achieve these lifestyle changes is difficult and has been addressed in the chapter on lifestyle modification (see Chapter 19). If all physicians would address lifestyle changes at EACH and every patient visit, meaningful change could eventually be achieved for many patients.
TABLE 20.1 Federal Resources on Complementary and Alternative Medicine for Providers and Patients
Federal Resources for Providers
National Center for Complementary and Alternative Medicine: nccam.nih.gov/health/providers
Online Continuing Education Series: Video lectures available for CME/CEU credits: nccam.nih.gov/training/videolectures
OCCAM website: cam.cancer.gov
Resources for Patients
National Center for Complementary and Alternative Medicine: nccam.nih.gov; Toll-free clearinghouse: 1-888-644-6226
NCCAM Time to Talk Tips: nccam.nih.gov/health/tips
Medline Plus: medlineplus.gov
OCCAM website: cam.cancer.gov
Food is a fundamental and essential element to the well-being of everyone. There is still a paucity of education around nutrition in medical training, and new research frequently changes recommendations, so keeping abreast of what to tell patients is difficult. Most people should be taking in five servings of vegetables and four servings of fruits daily. This may sound like a lot; however, when the appropriate serving size of either a fist or a deck of cards is taken into account, this may be easier to accomplish than on first glance.
Carbohydrate intake should be modified to include very few simple or refined carbohydrates and to maximize the amount of whole grains consumed. Fiber is essential, and taking in the recommended fruit and vegetable servings as well as plenty of whole grains has been shown to decrease the risk of diabetes, cardiovascular disease, and possibly colon and breast cancers.18
Women should be encouraged to consume plant sources of protein, such as soy. If they choose to consume animal sources of protein, fish and chicken should predominate and red meat should be consumed rarely.
High-quality fats are an important component of the diet. Poor-quality fats, such as trans fats, butter, and margarine should be eliminated from the diet entirely because they increase triglycerides and inflammatory mediators in the blood.19 This can lead to a prothrombotic state with an increased risk for cardiovascular disease.20 A greater propensity for increased endothelial inflammation arises after a high-fat meal in persons with abdominal obesity and hypertriglyceridemia.21 Olive, canola, and grape-seed oils are healthy alternatives to poor-quality fats. Omega-3 fatty acids have been shown to decrease cardiac death and all-cause mortality in coronary heart disease patients.21a Recommendations call for women to eat at least three servings of fatty fish, such as salmon or cod, or consider the addition of supplements with purified fish or flaxseed oils.22
Many “diets” may be found in the literature, and patients are likely to ask for recommendations about them. In general, the Dietary Approaches to Stop Hypertension (DASH) diet and the Mediterranean diet provide an excellent starting place for dietary interventions for patients. The Mediterranean diet is an example of a healthy diet that encourages high consumption of fresh fruits and vegetables as well as whole grains and healthy fats such as olive oil. Several good clinical studies have shown that women who follow the Mediterranean diet when combined with a healthy lifestyle and exercise have decreased all-cause mortality.23,24 Evidence has shown that this type of diet decreased incidence of cardiovascular disease,25 certain cancers,26 and obesity.27 More information can be found at http://dashdiet.org/ and http://www.mayoclinic.com/health/mediterranean-diet/CL00011/.25, 26, 27
Moderate-to-intense physical activity for 30 to 60 minutes a day is recommended for almost all patients. This can include housekeeping activities such as vacuuming, washing floors, and walking dogs as moderate activities and mowing lawns and jogging as intense activities. Many people are quite sedentary, and some forget that modifying simple activities can greatly increase caloric output. Simple habits, such as parking farther away from store entrances or taking the stairs can increase physical activity in sedentary patients—anything to get them moving! When making recommendations for patients to increase exercise, the doctor often finds it helpful to learn what the patient enjoys doing and to invite her to help set exercise goals that are attainable.
Mind-Body Interventions
The mind has a powerful connection to the body, so addressing spiritual and mental health is an important part of integrative medicine. Mind-body therapies focus on the relationships among the brain, mind, body, and behavior, and their effect on health and disease. These approaches encompass a large group of techniques such as hypnosis, meditation, yoga, biofeedback, tai chi, visual imagery, acupuncture, massage therapy, and spinal manipulation, just to name a few. As research expands, there is a growing body of evidence that suggests a variety of interactions between the central nervous system (CNS), the endocrine, immunity, and peripheral autonomic nervous systems that may provide insight into the mechanisms of action by various mind-body approaches.
More than 3000 studies have shown a benefit from relaxation.28 Thus, giving attention to behaviors that will reduce stress and create the relaxation response can positively impact well-being. These techniques can be taught and learned. Like most things, regular practice improves performance and has been shown to have long-lasting, positive effects on health.
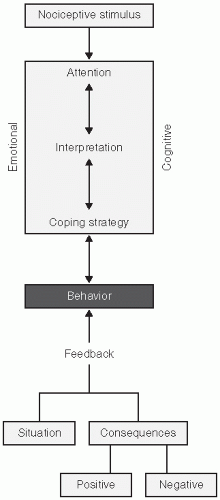
Mind-body approaches are used in a variety of conditions associated with chronic pain, although evidence of their efficacy varies. Pain perception occurs in many centers in the brain, including the regions that are involved with attention, beliefs, conditioning, mood, emotion, stress, and cognition (see Fig. 20.1). Mind-body approaches to chronic pain work at one or more of the levels of the experience of pain and may have synergistic effects.30 The feelings of stress, fear, and depression that often accompany chronic pain may amplify the perception of pain and the pain perceived may exist even in the absence of demonstrable tissue damage. A set of guiding principles relating to psychological factors and the management of pain has been created based on scientific evidence and is found in Table 20.2. A variety of mind-body interventions have been advocated for use in the management of chronic pain. The relaxation response may be associated with greater pain tolerance and mindfulness-based approaches may lessen the impact of the hypervigilance and emotional reactivity linked to the genesis of chronic pain and allow for the development of acceptance (not resignation) of chronic pain symptoms, making it easier to focus on other experiences, participation in valued activities, and pursuing personally relevant goals.31
FIGURE 20.1 Pain perception pathways. (Reproduced with permission from Linton SJ, Shaw WS. Impact of psychological factors in the experience of pain. Phys Ther. 2011;91:700-711.)
In one review of randomized trials using psychosocial interventions for chronic pain, group-delivered courses that had health care professional input showed more benefit.32 Some mind-body skills are easily used in general practice, whereas others may require more extensive training.
In an interesting randomized study, participants who listened to a guided imagery CD preoperatively reported less pain and anxiety postoperatively and were discharged earlier from the postoperative anesthesia care unit (PACU).33 Astin et al.34 reported that presurgical mind-body programs reduced pain, anxiety, drug requirements, and days in the hospital. Such low-risk and high-benefit interventions should become the standard of medical care. Other uses of mind-body therapies for various clinical conditions may be found in Table 20.3.
TABLE 20.2 Ten Guiding Principles Relating Psychological Factors to the Management of Pain
Treatment Phase
Number
Guiding Principle
Clinical Implications
Assessment
1
Psychological factors that may affect pain outcomes are not routinely assessed by many treating clinicians.
Better methods of screening and early intervention are needed to improve feasibility and utility in usual care settings.
2
Persistent pain naturally leads to emotional and behavioral consequences for the majority of individuals.
Psychological concepts of learning can be useful to provide empathy and support without reinforcing pain behavior.
3
Clients who are depressed or have a history of depression may have more difficulty dealing with pain.
A brief assessment of mood symptoms should be part of routine screening and intake procedures for pain conditions.
Treatment planning
4
Persistent pain problems can lead to hypervigilance and avoidance, but simple distraction techniques are not enough to counter these behaviors.
Clinicians should avoid inadvertent messages that escape or avoidance from pain is necessary in order to preserve function.
5
Individuals hold very different attitudes and beliefs about the origins of pain, the seriousness of pain, and how to react to pain.
Assessment and treatment planning should take into account individual differences in pain beliefs and attitudes.
6
Personal expectations about the course of pain recovery and treatment benefits are associated with pain outcomes.
Providing realistic expectations (positive, but frank and not overly reassuring) may be a very important aspect of treatment.
7
Catastrophic thinking about pain is an important marker for the development of long-term pain problems as well as for poor treatment outcome.
Clinicians should listen for expression of catastrophic thoughts and offer less-exaggerated beliefs as an alternative. A brief assessment might be part of routine intake procedures.
Implementation
8
Personal acceptance and commitment to self-manage pain problems are associated with better pain outcomes.
Overattention to diagnostic details and biomedical explanations may reinforce futile searches for a cure and delay pain self-management.
9
Psychosocial aspects of the workplace may represent barriers for returning to work while pain problems linger.
Return-to-work planning should include attention to aspects of organizational support, job stress, and workplace communication.
10
With proper instruction and support, psychological interventions can improve pain management outcomes.
Psychological approaches can be incorporated into conventional treatment methods but require special training and support.
From Linton SJ, Shaw WS. Impact of psychological factors in the experience of pain. Phys Ther. 2011;91:700-711.
Dietary Supplements
Plants have been used for thousands of years for medicinal purposes and all cultures use botanicals for purposes of healing. Over time, standardized pharmaceutical drugs have replaced herbal therapies in the United States, Europe, and other areas of the world. In the first half of the 20th century, herbs were included in the U.S. National Formulary and U.S. Pharmacopoeia.35 After 1962, herbal medicines were reassigned to the category of food supplements, which have a lower threshold of required evidence for demonstrating safety.
In 1994, Congress passed the Dietary Supplement Health and Education Act (DSHEA), which defined dietary supplements as a product containing one or more of the following: a vitamin, mineral, amino acid, herb, other botanical concentrate, metabolite, constituent, or extract, and it placed supplements in a category distinct from drugs. Supplements are required to carry the following statement on their labels: “This product is not intended to diagnose, treat, cure, or prevent any disease”; however, this does not preclude their manufacturers from making health claims, for example, “promotes good eye health.” Manufacturers of supplements are not required to prove efficacy, safety, or quality of their products prior to marketing or selling them. They are also not required to provide the FDA with any postmarketing data on adverse events. Although this requires the FDA to prove a product is unsafe or not effective and not many supplements have been removed from the market, some have; for example, ephedra, androstenedione, and PC-SPES. Adverse events may be reported to the FDA MedWatch program at 1-800-FDA-1088, online at www.fda.gov/safety/medwatch, by faxing 1-800-FDA-1078, or through the mail.
In 2007, the U.S. Food and Drug Administration (FDA) issued new rules that required good manufacturing practices (GMPs) for supplement makers to be phased in from 2008 to 2010. These rules required that supplements be properly labeled, free of adulterants, and made according to specified standards regarding equipment and personnel. There is still a great deal of flexibility for the manufacturers to choose the quality criteria they will follow, however. There is substantial variation in the quality of commercially available products in the United States as a result. Many things will determine the quality of a supplement, particularly one that is plant derived such as the plant species used, the parts of the plant that are used, harvesting and storage conditions, and processing. These variations may impact the supplements safety, efficacy, and clinical usefulness.
TABLE 20.3 Overview of Mind-Body Therapies for Various Clinical Conditions
EMG biofeedback or thermal biofeedback plus relaxation
Tension headache
Biofeedback
Guided imagery
B
C
Irritable bowel syndrome
Hypnosis
Guided imagery
A
C
Hypertension
Biofeedback
B
Thermal or electrodermal biofeedback best, add relaxation or cognitive therapy to biofeedback
Raynaud’s phenomenon (primary)
Biofeedback
B
Anxiety disorders
Mindfulness meditation
B
Depression
Mindfulness meditation
A
MBCT or MBSR
Insomnia
Mindfulness meditation
Biofeedback
Hypnosis
B
C
C
Progressive muscle relaxation and combination of mindbody therapies also shown effective
Urinary incontinence
Biofeedback
A
Stress, urge, mixed or post-prostatectomy
Fecal incontinence
Biofeedback
B
First-line therapy
Chronic constipation (pelvic floor dyssynergia)
Biofeedback
A
First-line therapy
Asthma
Biofeedback
Hypnosis
C
C
1 Level of evidence: A, high quality: consistent evidence from randomized trials or overwhelming evidence from other sources; B, moderate quality: evidence from randomized trials with important limitations or very strong evidence of some other form; C, low quality: evidence from observational studies or randomized trials with serious methodologic flaws.
Elkins G et al. Mind-body therapies in integrative oncology. Curr Treat Options Oncol. 2010 Dec;11(3-4):128-40. [PMID: 21116746]
Nguyen LT et al. Use of mind-body medicine and improved self-rated health: results from a national survey. Int J Person Centered Med North America. 2011 Sept; 1. http://ijpcm.org/index.php/IJPCM/article/view/111.
Wahbeh H et al. Mind-body interventions: applications in neurology. Neurology. 2008 Jun 10;70(24):2321-8. [PMID: 18541886]
In Europe, herbal medicine is often referred to as phytotherapy and it is commonly integrated with conventional medicines. German physicians receive training in medical school in herbal medicine and this is included in their testing for licensure. Regulation of herbal products in Europe is greater than in the United States and a 2004 EU directive requires manufacturers of nonprescription herbal products to register and license all products with the European Agency for the Evaluation of Medicinal Products. Premarket evaluations of efficacy and safety are required and postmarketing surveillance by the companies is required, as is the reporting of serious adverse events.
There have been reports of herbal medicines containing pharmaceutical agents; for example, PC-SPES was used for prostate cancer by some and was found to contain diethylstilbestrol (DES), warfarin, and indomethacin.36 Reports of contamination with lead, mercury, arsenic, and other heavy metals in imported herbal products have also been reported.37,38
Most Americans use dietary supplements, with usage rates ranging from 40 to 70% in the general population.39,40 In most reports, women use more dietary supplements than men; in at least one study, usage among elderly women was reported to be as high as 84%.41 According to one nationally representative survey, the most commonly used supplement is fish oil or other omega-3 supplements.42 In that same survey, the most common reason people used supplements were to “feel better” (41%), “improve overall energy levels” (41%), and to “boost your immune system” (36%). When asked if public health authorities declared the use of the supplement they were taking to be ineffective, only 25% of respondents said they would stop using it, a finding similar to an earlier 2001 study.43
Women often seek advice about supplements from their friends, family, and the Internet.44 The Office of Dietary Supplements (ODS) at the NIH (www.ods.od.nig.gov) offers information on individual vitamins, minerals, and other dietary supplements and a link to a new PubMed subset, “Dietary Supplements,” available online at http://ods.od.nih.gov/Research/PubMed_Dietary_Supplement_Subset.aspx.
Clerks at health food stores routinely advise patients about dietary supplements. In one study, a researcher posed as the daughter of a woman recently diagnosed with breast cancer and asked for advice from 40 separate health food stores in the area. In all instances, she was given advice about what supplements to take.45 In a more recent study, researchers reporting classic symptoms of type 1 diabetes asked for advice from health food store employees: 75% of the clerks recommended a natural supplement, only 25% of them recommended urgent physician evaluation, and 25% of them advised NOT to seek medical attention.46 Researchers found that fewer than half health food store clerks surveyed inquired about the use of other drugs and supplements before recommending St. John’s wort for depression, which is known to have some serious drug interactions.47
The use of dietary supplements to lose weight is extremely popular, but the efficacy for most of these supplements is not proven. Chromium is a supplement that has gained increasing attention for use in weight loss programs; it is an essential trace element, and in human tissues, is necessary for the metabolism of fats and carbohydrates. Reports suggest that chromium increases insulin sensitivity, may potentiate the actions of insulin at the receptor, decrease food cravings, and increase metabolic rate.48, 49, 50, 51 A recent review and meta-analysis showed that although there is a statistically significant difference in body weight and percentage of body fat between chromium use and placebo, the clinical relevance of this is unclear (weight loss was less than 5% of body weight), future clinical trials should last at least 16 weeks, and there are concerns with adverse events such as renal impairment, hepatotoxicity, vertigo, weakness, nausea, and vomiting.52, 53, 54
TABLE 20.4 Sources for Dietary Supplements
Organization
Online Website
American Botanical Council
http://www.herbalgram.org
Consumer Labs
http://www.consumerlabs.com
Health Canada
http://www.hc-sc.gc.ca
National Center for Complementary and Alternative Medicine (NCCAM)
http://www.nccam.nih.gov
National Nutritional Foods Association—Good Manufacturing Practices (GMP)
http://www.nnfa.org
National Sanitation Foundation International (NSF)
In light of the evidence that diets rich in fruits and vegetables, which are replete with various vitamins and antioxidants, are associated with a reduction in risk for cardiovascular disease (CVD), there is also strong interest in the use of vitamins and antioxidants as supplements to prevent CVD.55 Some estimates note that if fruit and vegetable intake were increased to 600 g per day, the worldwide burden of disease due to ischemic heart disease could be reduced by 31% and by 19% for ischemic stroke.56 Meta-analysis from randomized controlled trials looking at the efficacy of supplements in reducing or preventing CVD or cerebrovascular events show mixed results.57, 58, 59, 60 In a recent meta-analysis that included various subgroup analyses, Myung et al.60a found no evidence that the use of vitamin or antioxidant supplements were helpful in either the primary or secondary prevention of CVD.
Although the available evidence may be ambiguous and sometimes conflicting, providers should work with their patients as they make decisions regarding dietary supplements, be aware of resources that are reliable in order to evaluate the supplements in use or being considered, and should routinely ask about the use of dietary supplements in a nonjudgmental fashion because some women will not disclose their use because of fear of a negative response61 (Table 20.4). Most supplements and their safety and/or purported efficacies are associated with evidence that is conflicting, uncertain, or insufficient. Providers should counsel patients about this and the possible impact of unknown quality of the supplements should be emphasized, particularly because lack of regulatory reform in the supplement industry in the United States makes it impossible to make an informed recommendation for specific brands. Clinicians and patients should also be aware that the use of herbs and dietary supplements alone or concurrently with medications may increase the risk of adverse events. Herbs and supplements with St. John’s wort, magnesium, calcium, iron, and ginkgo appear to have the greatest number of reported interactions with medicines.62 Among medications, those that affect the CNS or the cardiovascular system, as well as warfarin, insulin, aspirin, digoxin, and ticlopidine have the greatest number of reported interactions with herbs and supplements. Flaxseed, echinacea, and yohimbe have the largest number of documented contraindications. Most of these adverse interactions are due to altered pharmacokinetics, particularly when the metabolism of cytochrome P450 enzymes is involved. There are some commercial applications and software programs available that will allow clinicians to analyze a patient’s entire drug and natural product usage to identify potential interactions.
Only gold members can continue reading. Log In or Register to continue