Choledochal Cyst
Ryan D. Reusche
Hibbut-ur-Rauf Naseem
HISTORICAL BACKGROUND
Choledochal cysts were first described by Vater in 1723.1
Anatomic variations of choledochal cyst were later classified by Alonso-Lej et al in 1959.2 Subsequently, Todani et al classified choledochal cysts into 5 major types and multiple subtypes. This is the most commonly used classification system today.3
Described in literature up through the 1970s a cholecystoenterostomy was considered a surgical management option for choledochal cysts.4,5
RELEVANT ANATOMY
Type I (most common): consists of dilatation of the common bile duct, which may be cystic, focal, or fusiform (subtypes A, B, and C, respectively)
Type II: a saccular diverticulum off the common bile duct
Type III: a cystic dilatation of the intramural portion of the common bile duct (may represent a duodenal diverticulum rather than a choledochal cyst)
Type IV-A (second most common): both intrahepatic and extrahepatic dilatation of the biliary tree
Type IV-B: Multiple extrahepatic cysts
Type V: “Caroli disease”; multiple intrahepatic biliary dilatations (Figure 20.1)
EPIDEMIOLOGY AND ETIOLOGY
Incidence: It varies depending on ethnic and geographic locations. There is higher incidence of choledochal cysts in Asian populations compared with other ethnicities.8
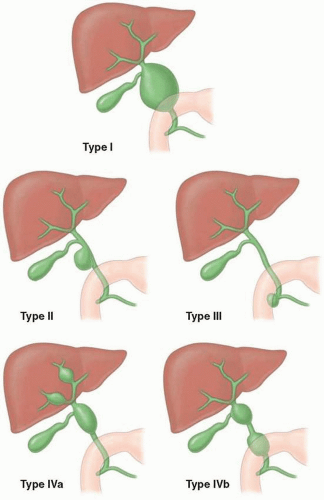 Figure 20.1 Artistic rendering of choledochal cyst types I-V and their prevalence. (Reprinted with permission from Lee EY. Pediatric Radiology: Practical Imaging Evaluation of Infants and Children. Philadelphia, PA: Wolters Kluwer; 2018.) |
Etiology: Many theories as to the exact etiology exist, but it is possibly multifactorial.
The most universally accepted theory is that pancreatic juice refluxes into the biliary system, causing increased pressure within the common bile duct that leads to ductal dilatation.12
They are associated with an anomalous pancreatobiliary junction with a long common channel (>15 mm).
Additionally, abnormal function of the sphincter of Oddi has been reported to predispose to pancreatic reflux into the biliary tree, which may be associated with choledochal cysts.13
CLINICAL PRESENTATION
Classic presentation: classic triad (seen in 10%-20% of patients)—palpable right upper quadrant mass, jaundice, and abdominal pain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


