Average life expectancy at birth for women in the United States has increased from 48 in 1900 to 80.4 in 2005.1 It is a relatively new phenomenon for women to spend a significant portion of their lives in the post reproductive state. As average life expectancy increases, so does the number of elderly Americans; by 2050, it is estimated that more than 20% of the population will be older than 65 years of age. In the United States, the most rapid growth is estimated to occur between 2010 and 2030, as the American “baby boomers” reach 65 years of age. Because women’s life expectancy is longer than men’s, the majority of this growing elderly population will be women.2 The average age of a woman at menopause is 51 years, and more than 90% of women are postmenopausal by 55 years of age.3 Many women are interested in information about how to best negotiate their post reproductive years and a large variety of literature is available on the topic in both the medical and lay press. As women spend more of their lives in the postmenopausal state, the changes associated with menopause are becoming better described and more fully understood. The continued expansion of this knowledge and the development and evaluation of lifestyle and screening recommendations as well as treatment options to optimize the health and well-being of this population is especially worthwhile given the expected continued growth of this population.
The menopausal transition and ensuing menopausal state has enormous health implications for a woman. Reproductive capabilities are most obviously affected, but menopause also has a potentially large impact on cardiovascular health, mood, musculoskeletal symptoms, bone mass and fracture risk, cancer risk, and cognitive function. Estrogen receptors are omnipresent in the human body. Separating the effects of menopause from those of the normal aging process can be a challenge for both patients and clinicians. This chapter reviews the important changes that accompany the menopausal transition and beyond, as well as the therapies and preventive strategies available for symptomatic relief and long-term disease prevention. As women spend more years in the postmenopausal state, this period in a woman’s life becomes an opportunity to promote healthy behaviors and improve the adoption of appropriate preventive measures and screening techniques (Table 24.1).
Whether to “treat” menopause with replacement of reproductive hormones (estrogen and/or progesterone and/or testosterone) has been a subject of much study and controversy since synthetic estrogen became available in the mid-20th century. Common clinical recommendations have ranged from regarding menopause as an estrogen-deficiency disease that should be treated with estrogen replacement therapy to prevent the otherwise inevitable “living decay”4 to treating symptoms only if absolutely necessary “for the shortest time with lowest dose possible”5 and all points in between. Current thinking on this topic is also reviewed in this chapter.
DEFINITIONS
The language we use to describe the menopausal transition has been historically varied in both definition and context. Because this is a transition all women experience if they live long enough, our patients often have their own conceptions regarding this time in their lives. Having well-defined language to describe this period in a woman’s life helps us to increase our patients’ understanding of this life event and also gives us a descriptive context for communication of research findings and clinical experience. As more study has been done of the natural history of the menopausal period, the following terms have been developed and used in this chapter. Although other symptoms, especially vasomotor symptoms, often accompany the transition to menopause, these definitions rely on menstrual patterns since hallmark of menopause is the cessation of menses.
Menopausal Transition: Menopausal transition describes the time from the onset of variations in the menstrual cycle and a rise in follicle-stimulating hormone (FSH) levels until 12 completed months of amenorrhea. This transition may also be referred to as perimenopause or climacteric and is a process that may occur over many years.6
Menopause: Menopause is the permanent cessation of menses secondary to the follicular depletion; it is considered to have occurred following 12 consecutive months of amenorrhea. This can occur naturally or be induced by bilateral oophorectomy, radiation to the ovaries, or by chemotherapy effects on ovarian follicular reserves.6
TABLE 24.1 Recommended Screening Tests and Immunizations in Healthy Menopausal Women
Screening Test
Age and Frequency
Purpose
Pap test
Every 3 years for low-risk women older than 30 years of age
Cervical cancer detection
Breast exam
Yearly by physician
Monthly self-exam
Breast cancer detection
Mammogram
Every 1—2 years after age 40 years; yearly after age 50 years
Breast cancer detection
Digital rectal exam
Yearly after age 50 years
Colorectal cancer detection
Flexible sigmoidoscopy
Every 3—5 years after age 50 years
Colorectal cancer detection
Densitometry
Age 65 years if low risk
At menopause if high risk
Osteopenia/osteoporosis detection
Lipid profile
Every 2 years after age 40 years
Cardiovascular risk assessment
Fasting glucose
Every 3 years after age 45 years
Diabetes detection
Sexually transmitted infections (STIs) and HIV testing
Yearly in high-risk patients
STIs and HIV detection
PPD skin testing
Yearly in high-risk patients
Tuberculosis detection
Immunizations
Influenza vaccine
Yearly after age 50 years, or earlier if high risk
Influenza prevention
Pneumococcal vaccine
Once at age 65 years, or earlier if high risk
Pneumonia prevention
Tetanus-diphtheria vaccine
Every 10 years
Tetanus and diphtheria prevention
Adapted from American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 452: primary and preventive care: periodic assessments. Obstet Gynecol. 2009;114:1444-1451.
Postmenopause: Postmenopause is the remaining life period of the woman after 12 consecutive months of amenorrhea.6
NATURAL HISTORY OF MENOPAUSE
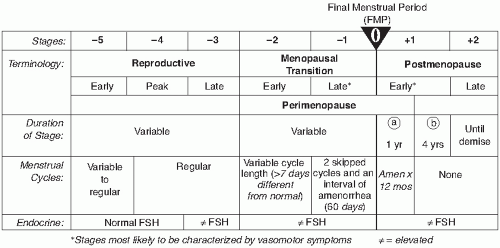
Several studies have been published describing the timing, duration, hormonal changes, and associated symptoms experienced by large populations of women passing thru this transition period.7,7a There is great variability in the age of onset and duration of the menopausal transition, but it appears that most women begin the transition at about age 47 and the median length from the onset of the transition to the final menstrual period (FMP) is 3.8 years.3 Staging systems such as the Stages of Reproductive Aging Workshop (STRAW) classification (Fig. 24.1) have been proposed attempting to describe the factors associated with the usual progression through the menopausal transition and to help predict how soon the FMP will occur. An intermenstrual interval of greater than 60 days is both predictive of the FMP within 2 years8,9 as well as current failure of ovulation.10
FIGURE 24.1 STRAW staging system. (Reprinted from Fertil Steril 2001;76[5], with permission.)
By definition, menopause is a diagnosis made in retrospect. The average age of permanent cessation of menstrual bleeding is 51.4 years.3 Factors associated with an earlier age of menopause include poor nutritional status, family history, vegetarianism, and living at high altitudes. Women who currently smoke appear to experience menopause 1.8 years earlier than nonsmokers. Alcoholism has also been linked to delayed menopause.11, 12, 13, 14, 15, 16, 17 While age at natural menopause is most likely influenced by genetic factors, and a number of genetic regions have been studied, as yet there is no clear understanding of which regions of the genome are involved with an individual’s menopausal timing.18
ENDOCRINOLOGY OF THE MENOPAUSE TRANSITION
A woman is born with all the ovarian follicles she will ever develop; over time, these follicles become depleted. When the number of follicles drops very low, inhibin levels decrease and activin rises.19 Negative feedback from the ovary to the pituitary diminishes, resulting in rising FSH levels.20,21 The initial elevation in FSH is first detectable only in the early follicular phase. During the early menopausal transition, in response to the increased FSH stimulation, estradiol levels fluctuate widely and can actually be higher than average levels found in women younger than 35 years of age.22,23 Estrogen levels do not begin a major decline until a year or so before menopause.24 During perimenopause, FSH levels vary significantly across cycles.25 Postmenopausal levels of FSH (>20 IU/L) may be seen despite the presence of menstrual bleeding, although luteinizing hormone (LH) levels remain in the normal range. Because of this variability of hormonal secretion during the menopausal transition, the diagnosis of perimenopause and menopause is not made based on laboratory studies but instead depends on the patient’s individual symptoms and menstrual history. However, elevation in FSH in the early follicular phase has been associated with poor prognosis for future fertility and success of efforts at induction of ovulation.26
After menopause is completed, there is a 10- to 20-fold increase in FSH (>25 IU/L) and about a three-fold increase in LH (>30 IU/L).27 Almost all postmenopausal production of estrogen is derived from the peripheral conversion of androgens.28 Although reduced from earlier premenopausal levels, the ovary still secretes androstenedione and testosterone in the early postmenopausal years.29 In the later postmenopausal years, circulating androgens are almost all derived from the adrenal gland.
This natural decline in estrogen is responsible for the various physiologic effects described in the following sections.
SYSTEMIC AND SYMPTOMATIC EFFECTS OF MENOPAUSE AND THE MENOPAUSE TRANSITION
Fertility
For many perimenopausal women, menstrual cycle length increases and anovulation becomes more prevalent, particularly in the 2- to 8-year period prior to menopause. During this time, there is an accelerated rate of loss of ovarian follicles until the supply is finally depleted.30 Although these changes reflect increasing difficulty in achieving pregnancy, pregnancy can and does occur in perimenopausal women. Approximately 51% of pregnancies in this age group are unintended.31 It therefore remains important during the menopausal transition to discuss the need for effective contraception with heterosexually active women not interested in becoming pregnant. For those interested in achieving pregnancy in this age group, FSH measurement on the third day of a naturally occurring menstrual cycle is predictive of ovarian reserve and response to ovulation induction. Elevated day 3 (or days 2 to 5) FSH levels are associated with a poor prognosis for success with ovulation induction.32
Menstrual Cyclicity and Abnormal Bleeding
During the reproductive years, normal menstrual cycles typically occur every 21 to 35 days. Variation in the timing, duration, and amount of menses signals the beginning of the menopausal transition. In perimenopause, a reduction in progesterone production during the luteal phase is common. This reduction coupled with normal or even increased levels of estrogen production leads to hormonal imbalances and may be responsible for the menorrhagia some patients report during perimenopause. In early perimenopause, cycle length may shorten by 2 to 7 days secondary to a shortened follicular phase.33 As the perimenopause progresses, cycles becomes increasingly irregular. As menopause approaches, menstrual flow may become lighter, and episodes of spotting may become more prevalent.23
Therefore, “abnormal” bleeding is common during the transition through menopause. It most often occurs as a result of the fluctuating hormonal environment and anovulation. Failure to ovulate regularly causes periods of unopposed estrogen stimulation of the endometrium. Prolonged estrogen exposure leads to proliferation, which can eventually lead to episodes of irregular and even heavy bleeding. Such unopposed estrogen stimulation also can increase the risk for hyperplasia and endometrial cancer. Heavy bleeding, however, has been shown to correlate less with anovulatory cycles and more with obesity and leiomyomata.33 The need to evaluate heavier or more frequent bleeding commonly arises in the perimenopausal woman. After pregnancy, endocrine etiologies are ruled out, biopsy is performed. Office endometrial biopsy is generally well tolerated and has been shown to be more than 90% sensitive for detecting endometrial cancer.34 Transvaginal ultrasound with or without saline infusion may be used to evaluate the endometrium. In postmenopausal women, endometrial sampling is recommended if the endometrial stripe is thicker than 4 mm.35
Office diagnostic hysteroscopy is also a tool for the evaluation of the endometrium and the uterine cavity. Premedication with misoprostol may facilitate ease of cervical dilatation when cervical stenosis limits endometrial evaluation with biopsy and/or hysteroscopy.36 A dilatation and curettage (D&C) with hysteroscopy is recommended for women with postmenopausal bleeding when an office biopsy and/or hysteroscopy is not possible and endovaginal ultrasound does not provide reassurance. In perimenopausal women, endometrial evaluation via ultrasound is best performed immediately after completion of menses because endometrial thickness can vary with a normal menstrual cycle. Because of normal cyclic variations in endometrial thickness in perimenopausal women, the use of endometrial thickness for exclusion of endometrial pathology is of limited use prior to achievement of postmenopausal status.
In addition to excluding endometrial hyperplasia and cancer, endometrial biopsy provides a “snap shot” of hormonal influences on the endometrium and can be used as a guide to treatment recommendations for bothersome bleeding patterns. In addition, the external genitalia, vagina, and cervix should be thoroughly inspected and a Papanicolaou (or Pap) smear considered to exclude other causes of bleeding.37 For a more thorough discussion of abnormal bleeding, see Chapter 2.
Once pathology has been excluded, anovulatory bleeding may be treated hormonally. Use of a traditional postmenopausal hormone therapy regimen (estrogen with progestin) in the perimenopausal woman is less likely to regulate bleeding patterns caused by anovulation and/or commonly concurrent adenomyosis or fibroids. Therefore, this approach is not recommended. Monthly progestational therapies in conjunction with an appropriate nonhormonal contraceptive method or a combination hormone contraceptive (e.g., oral contraceptives, the contraceptive patch, or vaginal contraceptive ring) are optimal therapies. If not contraindicated, combined hormonal contraception preparations regulate bleeding, relieve vasomotor symptoms, reduce ovarian cancer, and maximize bone density in women.37 Depo-medroxyprogesterone acetate (MPA) has been used to control bleeding and also to provide contraception, but calcium intake needs to be maximized. The levonorgestrel containing intrauterine system (LNG-IUS) was approved in 2009 by the U.S. Food and Drug Administration (FDA) for treatment of heavy menstrual bleeding in women also desiring contraception. It is a safe and convenient option. There is little support in the literature for cyclic MPA administration during the menopausal transition, despite its popularity.38
Cessation of combined contraceptive therapy can occur at ages 50 to 51 years. Some authorities recommend tapering to combined contraceptive to decrease the symptoms from abrupt estrogen withdrawal. This can be done by tapering one pill per week or even cutting patches into halves or quarters. Heterosexually active patients wishing to avoid pregnancy should be advised to use “backup” method when discontinuing hormonal contraception until they have experienced several months of amenorrhea. The decision to initiate postmenopausal hormone therapy once menses have stopped should be individualized depending on symptoms, individual risk factors, and patient goals.
Vasomotor Symptoms
Vasomotor symptoms are the most characteristic symptom of the menopausal transition and can be very troubling to women. The sudden sensation of extreme heat in the upper body, particularly the face, neck, and chest is referred to as a “hot flush” or “hot flash.” It is estimated that 15 to 63% of perimenopausal women experience hot flushes, with a higher percentage of women reporting vasomotor symptoms in the later part of the menopausal transition.32,39, 40, 41, 42 Although hot flashes are a common phenomenon for up to 80% of American women at some point during the menopausal transition,43 they are more common in women with increased body mass, lower exercise levels, smokers, and women with a history of premenstrual dysphoric disorder or depression.44 There is also wide ethnic variation in occurrence of vasomotor symptoms in different ethnic groups, ranging from reported 0% in Mayan women in Mexico to 80% of Dutch women.45
Hot flashes are related to the timing of the last menstrual period as menopausal symptoms are found to be most severe in the late perimenopausal and early postmenopausal stages. As vasomotor symptoms increase in severity, so do the severity of atypical complaints (e.g., tenseness, irritability, lack of self-confidence, headache, muscle or joint pain, tiredness on waking).46 The severity and duration of hot flashes among perimenopausal women is highly variable, although they are usually more frequent and more severe at night and are more likely to occur prior to and during menstrual bleeding.3 Hot flashes are not correlated or directly related to endogenous estrogen levels.
Usually, hot flashes last 6 months to 5 years with an average duration of 2 years after the FMP.49 Some women report bothersome hot flashes for up to 15 years after menopause.47,48 When estrogen therapy is discontinued, vasomotor symptoms frequently resume. When helping guide women through this transition time, it can be helpful to emphasize the time limited nature of vasomotor symptoms without treatment. In general, these symptoms are most severe and bothersome in the perimenopausal and immediate postmenopausal period months and become more tolerable as time after the FMP lengthens.47 Although vasomotor symptoms can be bothersome to women, not all women find this phenomenon to be life limiting enough to require treatment. Sleep disturbance caused by night sweats can, however, affect mood and quality of life. Vasomotor symptoms also tend to be more severe in women who undergo more abrupt iatrogenically induced menopause secondary to premenopausal oophorectomy, radiation, or chemotherapy.49
The pathophysiology of hot flashes is not fully understood. Thermoregulation in humans depends on three major cooperating factors: the central nervous system, the body core and the peripheral vascular system.50 With a decline in estrogen production, the thermoregulatory center in the brain becomes unstable, leading to an acute activation of the sympathetic nervous system and peripheral vasodilatation with subsequent sweating, which is often followed by a compensatory cooling mechanism and even shivering. Hot flashes may also be accompanied by an accelerated heart rate and feeling of anxiety.51 While a very common symptom accompanying the menopausal transition, vasomotor symptoms can also occur in other conditions, such as diabetes or thyroid disease, pancreatic tumors, leukemias, pheochromocytoma, carcinoid syndrome, certain drugs, neurologic disorders, and in reaction to nitrites or sulfites.52
Therapeutic Options
Since the World Health Initiative study, many patients and practitioners have shied away from hormone replacement therapy (HRT). It is important to remember that it had a mean age of 63 years and that only 3.5% of women were 50 to 54 years old. Also, the risk of breast cancer did not increase in the combined estrogen-progestin group until the fourth year. Several well-designed studies have shown the efficacy of oral estrogen therapy over placebo in relief of vasomotor symptoms in women passing through the menopausal transition. Currently, short-term therapy with estrogen (2 to 3 years but not more than 5 years) is reasonable. Both frequency and severity of both night sweats and day time hot flashes are reduced by estrogen therapy. Multiple estrogen doses as well progesterone regimens have been shown to be effective.53 Other studies have also demonstrated the effectiveness of transdermal54 and higher dose transvaginal estrogens in for relief of vasomotor symptoms.55 Relief of vasomotor symptoms is not immediate for all women. It may take up to 4 weeks before symptom relief occurs.56
There is some evidence that a combination of estrogen and androgen may alleviate symptoms in women with refractory vasomotor symptoms.47 It appears that lower doses of estrogen are required when androgens are added.57,58
Progestins alone also appear to be an effective treatment for hot flushes. A 74% reduction in vasomotor symptoms has been demonstrated with doses of 10 to 20 mg/day of oral MPA (or 150 mg intramuscularly every 3 months), or 20 mg twice a day of oral megestrol acetate reduced symptoms in 85% of patients.59,60 In addition, norethindrone and norethindrone acetate in doses between 1.2 and 5 mg have been shown to be effective in relieving hot flushes in younger women undergoing gonadotropin-releasing hormone (GnRH) agonist therapy.61
Selective serotonin reuptake inhibitors (SSRIs), selective norepinephrine reuptake inhibitors (SNRIs), and gabapentin have shown some promise in treating vasomotor symptoms. Studies have compared these drugs favorably with placebo but have not shown the same level of effectiveness as estrogen therapy in the relief of hot flushes.62,63 These drugs also have not been approved by the FDA for treatment of vasomotor symptoms. The mechanism of the effectiveness of SSRI/SNRIs remains unclear, but it is understood that serotonin receptors in the hypothalamus are involved in temperature regulation.64 Based on double-blinded, randomized controlled trials, venlafaxine (Effexor XR) therapy for hot flashes can be started at a dose of 37.5 mg/day. The dose can be increased to 75 mg if needed but doses higher than 75 mg/day seem to have more toxicity but are not associated with greater efficacy.65 A similar trial with fluoxetine (Prozac), 20 mg/day, also demonstrated a significant reduction in hot flashes, although its effect seemed more modest than that seen with venlafaxine.66 Another more recent trial demonstrated the efficacy of paroxetine controlled release (Paxil) at doses of 12.5 mg/day or 25 mg/day.67 Paroxetine should not be used in women taking tamoxifen because it decreases metabolism of tamoxifen to its active metabolite and may therefore decrease tamoxifen’s effectiveness. Other new antidepressants such as escitalopram68 and desvenlafaxine succinate69 also have data to show they are more effective than placebo in the relief of hot flushes. Although generally welltolerated drugs, side effects of SSRI and SNRIs include nausea, difficulty with sleep, and dry mouth. In addition, SSRIs may have sexual side effects with inhibition of orgasm. These drugs should be withdrawn gradually when discontinuing to avoid withdrawal symptoms.70 Gabapentin (Neurontin) has been shown to significantly reduce hot flashes. Common side effects included somnolence and dizziness. It appears to be more modest in its impact on hot flashes than SSRIs.71
Historically, other medications have been used for treating hot flashes (e.g., Bellergal), but these are associated with limited efficacy and/or toxicity.72, 73, 74 Transdermal clonidine (100-µg patch changed weekly) has been used but is only slightly more effective than placebo.75 With other currently available effective therapies, treatments with limited effectiveness and/or frequent side effects are of mostly historical significance.
Weight loss and regular exercise may be helpful in reducing bothersome hot flashes. Dressing in layers, keeping bedroom temperatures cool, and avoiding alcohol and caffeine are also recommended as lifestyle interventions to reduce hot flashes. Alternative therapies for vasomotor symptoms are also discussed in Chapter 20.
Genitourinary Atrophy
Although vasomotor symptoms often are experienced early in the menopausal transition, the effects of estrogen deficiency on the genitourinary tissues are usually later in onset. Also, while vasomotor symptoms tend to decrease with time after the FMP, frequency and severity of genitourinary atrophy increase as time from the FMP progresses. Estrogen presence makes the vaginal mucosa thicker and surface epithelial cells richer in glycogen. Surface epithelial glycogen helps promote the presence of lactobacilli in the vagina and therefore maintenance of normal vaginal pH. The maintenance of normal vaginal pH is an important defense mechanism against vaginal infection. Lower estrogen levels lead to thinner, paler, and dryer vaginal mucosa, which can lead to a sensation of dryness, irritation, and itching. Lack of estrogen can also affect the collagen in the vaginal walls with consequent loss of elasticity and a decrease in vaginal caliber, especially at the introitus, as well as a decrease in vaginal length. All of these changes may lead to the experience of pain with sexual activity, especially vaginal penetration.
The thinner vaginal mucosa is also more susceptible to traumatic injury from sexual activity or even from friction with washing and wiping after urination or bowel movements. Atrophic vaginitis, presenting with acute onset burning and watery discharge, can occur as well. Exposure to previously innocuous chemicals found in some soaps and detergents can become a source of irritation. Because the epithelium lining the urinary tract are also estrogen dependent, dysuria, urinary frequency and urgency, as well as increased susceptibility to urinary tract infection may also occur as a consequence of lower estrogen levels after menopause.76,77
While nearly all women note a change in vaginal secretions after menopause, at least 50% of postmenopausal women experience some form of bothersome genitourinary symptoms.78 These symptoms can significantly affect a woman’s sexual, emotional, mental, and physical quality of life, resulting in social isolation and low selfesteem.79 Atrophy symptoms are underreported and may often only be elicited with direct questioning about sexual comfort, urinary function, and vaginal sensation. As women’s life expectancy increases, increased attention needs to be paid to the physiologic but often bothersome genitourinary changes accompanying the postmenopausal state. While gross atrophic changes in the external genitalia and vaginal mucosa are often obvious on exam, it is still important to rule out other causes such as vaginal infection or chemical irritation when women present with symptoms of vaginal irritation and/dyspareunia. A careful history regarding potential exposure to irritants as well as measurement of vaginal pH and microscopic examination of vaginal secretions is indicated. Examination and wet mount findings seen with atrophic change are summarized in Table 24.2. When examining postmenopausal women, external skin changes from atrophy can be difficult to distinguish from dystrophic, dysplastic, and neoplastic changes. Biopsy is often indicated to rule out more serious pathology, especially if skin changes do not respond to topical estrogen therapy.
Therapeutic Options
Genitourinary atrophy symptoms are clearly related to level and duration of estrogen deficiency. These symptoms are less common in postmenopausal women being treated with systemic estrogen therapy, with or without addition of progesterone. However, the amount of systemic estrogen needed to satisfactorily treat vasomotor symptoms may not be enough to treat atrophy symptoms.80 Conversely, local treatment of atrophy symptoms with vaginally applied estrogens will usually not cause enough systemic absorption to treat vasomotor symptoms. The effectiveness of vaginal estrogen treatment for atrophy symptoms has been well documented.81 Current vehicles available in the United States for localized vaginal estrogen treatment include vaginal creams, vaginally inserted tablets, and vaginally inserted long-acting rings (see Table 24.3). All are effective and in general well tolerated with few systemic side effects when used at doses intended for treatment of atrophy. Each currently available option has advantages and disadvantages. While creams have the most flexibility in dosing options, women often find them messy to use and may have issues with cleaning and reusing the applicator. Vaginally inserted estradiol containing tablets currently have two dosing options are less messy to use and come with individual applicators for each dose. Usual maintenance dose for both cream and tablets is twice weekly, an interval that may be more difficult to comply with. Estradiol containing rings are inserted vaginally and changed every 3 months. Although this dosing interval is more convenient, many women are not comfortable inserting and/or retaining the ring.
TABLE 24.2 Vaginal Atrophy Findings
Microscopy
Increased basal/parabasal, decreased superficial cells May see increased WBC and RBC from trauma
Larger nuclei; less cytoplasm; smaller, rounder epithelial cells; absence of other pathogens (i.e., yeast, Trichomonas, clue cells)
pH of vaginal secretions
>5
Gross appearance
Mucosa thin, flat, shiny; minimal secretions or thin watery secretions
Labial fusion at midline and/or laterally
Shrunken labia
Introital narrowing
Fissures superficial at introitus
WBC, white blood cell; RBC, red blood cell.
TABLE 24.3 Vaginal Estrogen
Medication
Dosing Interval
Advantage
Disadvantage
Vaginal estradiol tablet 25 mcg or 10 mcg
Initiate daily for 2 weeks then maintain at twice weekly
Less messy than cream, multiple doses available
Disposable applicator with each dose
May be difficult to remember twice weekly dosing
Cream— estradiol or conjugated estrogen
Initiate daily for 2 weeks then maintain at twice weekly
Can adjust dose Reusable applicator difficult for some patients to clean
Can be used externally for vulvar symptoms
May be difficult to remember twice weekly dosing
Estradiol vaginal ring
Change every 3 months
Only needs attention every 3 months
Reluctance to use retained ring
Systemic absorption of vaginally applied estrogens is a concern, especially in regard to elevation of risk of endometrial hyperplasia and cancer with prolonged unopposed estrogen stimulation of the endometrium. To date, studies of the endometrial effects as well as other side effects indicating systemic absorptions (i.e., breast pain and tenderness) of standard doses of vaginal estrogen-containing rings, creams, and tablets have been reassuring for the most part. In isolated studies, vaginal bleeding and breast tenderness and endometrial effects have been associated with use of conjugated equine estrogen (CEE)-based creams but other studies have not confirmed these effects.82 To date, there is no evidence that standard doses of vaginal estrogen for atrophy increases breast cancer risk or risk of recurrence in breast cancer survivors. However, this area has not been well studied. Studies do show much lower to absent systemic absorption of vaginal estrogens at standard doses and vehicles used for atrophy treatment as compared to systemic oral or transdermal administration.83 While systemic use of hormonal therapy for the treatment of menopausal symptoms remains controversial, vaginal estrogen use appears to be a safe and effective option for treatment of the very common symptoms caused by postmenopausal genitourinary atrophy.
Sexual Function
Female sexuality and sexual function is a complex blend of physiologic function, individual sexual identity, and other psychological influences. Definition of female sexual dysfunction (FSD) during and after the menopausal transition is not “one size fits all” but rather an individualized diagnosis that needs to encompass physical, psychological, and relationship aspects. Despite the popular belief that sexuality is not a part of an elderly person’s life, studies show that between 50 and 80% of older people have an interest in sex or are sexually active.84 It appears that the degree of continued sexuality activity depends on the physical condition of each partner and the strength of their relationship.85,86
Several definite changes affecting sexual function occur with the onset of menopause. Declining estrogen levels result in decreased vaginal lubrication and genital atrophy. Intercourse may be uncomfortable and associated with the sensation of burning, irritation, and spotting. Lubricants, estrogen therapy (vaginal and/or systemic), and regular sexual activity alleviate these symptoms.87 In addition to improving lubrication and elasticity of the vaginal mucosa, estrogen improves blood flow to the vagina and clitoris and modulates the sensory threshold in the vagina and external genitalia.
While atrophy symptoms can be fairly easily treated (see earlier discussion), understanding the effect of menopause on libido or sexual desire is more complex. Loss of libido is noted to occur and be problematic for many postmenopausal women.88 There is some evidence that hormone therapy results in improved arousal and sexual desire.89,90 Data regarding the effect of oral testosterone on sexual activity, satisfaction, and orgasm are mixed.90,91 Recent meta-analysis looking at the use of testosterone in addition to estrogen therapy concluded that adding testosterone to hormone therapy regimens in postmenopausal women seemed to improve sexual function.92 However, to date, in the United States, there is no commercially available FDA-approved testosterone for women except when used in combination with oral estrogens (see Treatment section). Large, randomized controlled trials examining the utility of a testosterone matrix patch for women for the treatment of sexual dysfunction during menopause are currently underway. Efficacy of the testosterone patch in combination with hormonal therapy has been shown in improving total satisfying sexual activity when compared to placebo in surgically and naturally menopausal women with the diagnosis of hypoactive sexual desire disorder (HSDD).93,94 In addition, studies of the testosterone matrix patch in postmenopausal women with HSDD not using hormone therapy showed increased desire and satisfying sexual experiences. Vaginal bleeding occurred more in treatment than placebo group but no endometrial hyperplasia or cancers were found on subsequent testing.95 Although short-term study of transdermal testosterone supplementation for the treatment of postmenopausal HSDD is encouraging, long-term safety and effectiveness data for exogenous androgens in women are still needed.
Oral dehydroepiandrosterone (DHEA) and dehydroepiandrosterone-sulfate (DHEA-S) supplements are available in the United States over the counter in varying doses, but there are no national quality control standards or oversight for these products. The bioavailability of DHEA-S varies by manufacturer. Results on the use of these androgens for menopausal symptoms and sexual dysfunction have been conflicting.96,97
Other medications have been studied for effectiveness with postmenopausal HSDD in women. Studies of sildenafil have yielded conflicting results. Dopaminergic drugs, such as bupropion, have been studied as well without conclusive results.98 It is important to remember that many factors can contribute to HSDD in both pre- and postmenopausal women. Chronic diseases and their medical treatments as well as underlying depression can affect a woman’s individual sexual desire and response. Issues in relationships can also influence sexual desire and response. As the population of postmenopausal women grows, we can expect more attention to the options available for postmenopausal women with issues with sexual function and desire.
Skin
With aging, the amount of collagen declines and thinning of the skin occurs; this results in decreased elasticity, wrinkling, and dryness. Because skin contains estrogen receptors, declining estrogen levels are believed to play a role in the skin changes that occur after menopause.
Several studies reveal that either systemic or topical estrogen treatment can protect a woman from these changes.99, 100, 101, 102, 103, 104 One observational study of 3875 postmenopausal women found that ever-users of estrogen were 30% less likely to suffer from dry and wrinkled skin than never-users.102 There is some evidence that continuous hormone therapy (HT) is associated with greater skin thickness than sequential administration.103 Avoidance of sun exposure, especially in women with fairer skin tones, improves skin quality. Commercially available moisturizers and exfoliates are also available both over the counter and by prescription. A thorough discussion of treatment options for skin aging is beyond the scope of this chapter.
Cardiovascular Disease
Cardiovascular disease (CVD) is the leading cause of death in women in the United States. In 2006, 1 in 2.8 deaths in American women was from CVD, whereas only 1 in 4.5 deaths was from cancer. More women in the United States die from heart disease than from the other leading causes of death including cancer, chronic lower respiratory diseases, Alzheimer disease, and accidents combined.104
After menopause, women’s risk for coronary heart disease (CHD) rises. Postmenopausal status is counted with the same importance as male sex in the National Cholesterol Education Program (NCEP) risk factors for CHD. The major risk factors for CHD can be divided into modifiable and nonmodifiable factors (Table 24.4).105
The strongest predictor of CHD in women is low high-density lipoprotein (HDL) cholesterol.106 Diabetes and dyslipidemia have been identified as more powerful risk factors in women compared with men.107 In fact, women with diabetes lose their premenopausal estrogen advantage and are at equal risk as men of developing coronary artery disease (CAD) in their forties.108
Metabolic syndrome characterizes commonly grouped risk factors associated with both CHD and type 2 diabetes. This syndrome results partly from heredity but is strongly influenced by obesity and inactivity. The prevalence of metabolic syndrome in the United States was 32.6% in women older than 20 years of age between 2003 and 2006.104,109 The American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement110 defines the diagnosis of metabolic syndrome when three or more of the following five risk factors are present:
Fasting blood sugar over 100 or active treatment for elevated blood sugar
HDL <50 (for women) or active treatment for elevated lipids
Triglycerides >150 or in treatment for elevated triglycerides
Waist circumference >88 cm (for women)
Blood pressure >130/85 mm Hg or active treatment for hypertension
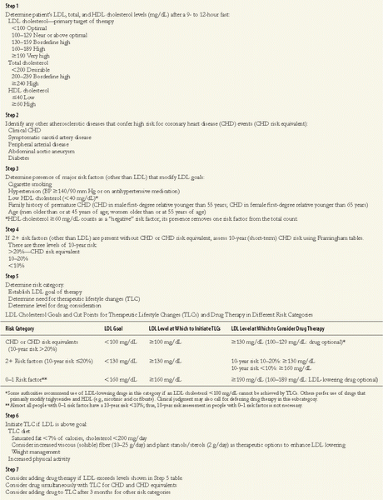
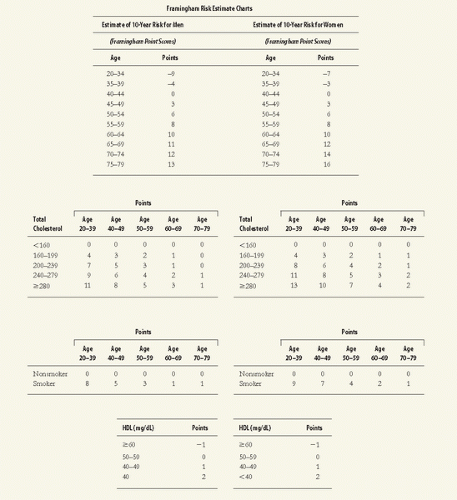
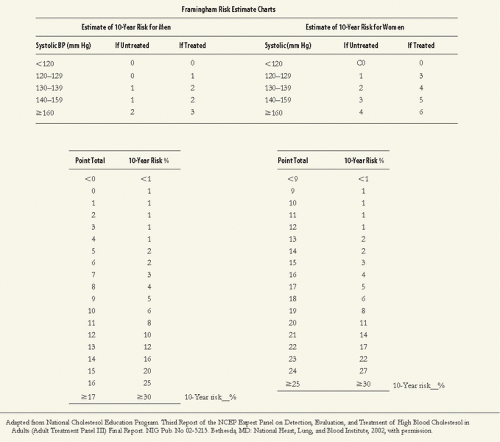
Women should be screened for hyperlipidemia through a fasting lipid profile, which should include total cholesterol, low-density lipoprotein (LDL), HDL, and triglyceride levels (Table 24.5). In addition, elevation of serum C-reactive protein was found to be a strong independent risk factor for CHD in the Women’s Health Initiative (WHI).111
TABLE 24.4 The Major Risk Factors of Coronary Heart Disease
Modifiable
Nonmodifiable
Elevated LDL Low HDL (less than 50) Elevated triglycerides
Increasing age (older than 55 years of age)
Hypertension
Male sex
Diabetes
Family history of premature CHD (first degree younger than the age of 65 years in women, younger than 55 years of age in men)
Although the goal of therapy for dyslipidemia depends in part on risk factors, the primary goal is reduction of LDL cholesterol. Statins are the first-line therapy for lowering LDL, and clinical trials have demonstrated a marked reduction in clinical cardiovascular events in women using cholesterol-lowering drugs.112 For women, measurement of non-HDL-cholesterol (HDL-C) by subtracting HDL from total cholesterol may give a better measurement of the amount of LDL lipoprotein particles than LDL-cholesterol measurement. This is because non-HDL-C measurement takes triglyceride levels and insulin resistance important in women’s risk valuation into the calculation. Treatment with statins should be considered for at-risk women with non-HDL-C >120 and for very high-risk women with non-HDL-C >80.113 Recent data also suggests that statin treatment in men and women with LDL <130 and elevated C-reactive protein over 2.0 mg/L reduced CVD endpoints of myocardial infarction, stroke, and death from CVD.114 Control of any elevation of blood sugar and treatment of underlying hypertension are also important in CHD risk reduction strategies. In addition, recommending modification of modifiable risk factors by encouraging weight loss and physical activity as well as smoking cessation is applicable to all women.
Prior to the publication of the results of the combination treatment arm of the WHI study in 2002, most observational studies seemed to indicate that postmenopausal HT reduced CHD risk. Initial WHI data, however, showed an elevation of risk of nonfatal myocardial infarction (MI) in postmenopausal women treated with combination HT.5 More recent analysis of the WHI data has suggested that elevation in risk for women taking HT may be limited to women initiating HT remote from menopause. In addition, other randomized studies of HT suggest no increase (and possible reduction) in CHD risk when initiated less than 10 years after menopause.115
Stroke and Venous Thromboembolic Events
Stroke is the third leading cause of death in the United States and affects one in five women. Although the incidence for stroke is about the same for men and women, at all ages, more women will die of stroke than men. Stroke rate doubles each decade after age 55 years. The most common type of stroke is atherothrombotic, accounting for 61% of all strokes. These strokes usually occur at atherosclerotic sites and lead to ischemic injury. The second most common type of stroke is cerebral embolus, accounting for 5 to 14% of all strokes.116 Risk factors for stroke include age, race, gender, and family history. A positive family history of stroke or transient ischemic attack almost doubles the risk of stroke. African Americans have the highest rates of stroke. Many studies have looked at the relationship between menopause and postmenopausal HT and stroke with varying results. Different studies comparing postmenopausal women taking HT have shown no effect, increased, and decreased risk of stroke. Those showing increased risk of stroke with the use of HT (including the WHI) have demonstrated an increase in thrombotic but not hemorrhagic stroke. As with other cardiovascular-related risk elevation in the WHI data, risk elevation seems to be clearer in older women who started HT remote from menopause. In addition, transdermal estrogen therapy may have less of an effect on stroke risk than oral HT (see Treatment section).117
In general, lifestyle interventions that decrease CVD risk in general such as exercise, weight loss, smoking cessation, and optimum management of diabetes and hypertension are strategies to decrease risk of stroke as well. Low-dose aspirin treatment is effective in decreasing stroke risk in all women older than 65 years of age and is also recommended for higher risk women younger than 65 years of age.
Venous thromboembolism (VTE) is the general term that includes deep vein thrombosis (DVT) and pulmonary embolism (PE). VTE has a yearly first-time incidence in the United States of about 100 cases per 100,000 persons. The incidence varies by, and increases with, age; there are approximately 500 cases per 100,000 (0.5%) in people 80 years of age and older. Of patients with VTE, close to two-thirds have DVT alone and about one-third concomitant with PE.76 VTE has a high recurrence rate, especially in the first few months after the initial event; the recurrence rate at 6 months is approximately 7%.118 The classic triad of risk factors for VTE is hypercoagulability, stasis, and endothelial injury. However, in 25 to 50% of patients with first-time VTE, no identifiable risk factors exist.118
Risk factors for VTE may be general, acquired, or inherited. Known heritable mechanisms include antithrombin deficiency and protein C and protein S deficiencies. Although it is important to identify these conditions because of the heightened risk of VTE, their overall contribution to the incidence of recurrent VTE is less than 10%.119 Most activated protein C resistance is due to a mutation in the factor V gene, also known as factor V Leiden. Elevated levels of specific coagulation factors are associated with increased risk of VTE, particularly factor VIII. The exact relationship between hyperhomocysteinemia and VTE risk is not currently known.118 While menopausal status has not been shown to be a factor in elevation of VTE risk, VTE risk was elevated in the HT treatment arm of the WHI study, especially in the first year of treatment.5 Prevention of VTE is centered on avoidance of high-risk circumstances such as prolonged immobility and prophylaxis of appropriate people with anticoagulation after a VTE event and surrounding high-risk surgical procedures. Further discussion of the prevention of VTE is beyond the scope of this chapter.
Osteopenia/Osteoporosis
Osteoporosis and its associated increase in fracture risk is a common problem for women as they age (Table 24.6). For example, it is estimated that a white American woman at age 50 years has a 40% risk of suffering an osteoporosis-related fracture in her lifetime.120 The hip, vertebrae, and wrist are the most common fracture sites in osteoporotic women. It is estimated that two-thirds of osteoporosis fractures occur after age 75 years.121 Hip fractures are associated with a 25% increase in mortality in the year after the fracture. In addition, after hip fracture, 50% of women suffer some long-term loss of mobility. Hip fracture is commonly the event that causes a woman to lose her independence; 25% of women require long-term care after hip fracture. Only 40% of hip fracture patients regain their previous level of mobility, and one-third will break the opposite hip in the future.122 Vertebral fractures can also cause pain, loss of height, and kyphosis. Thoracic vertebral fractures can cause restriction on respiratory and digestive functions.123
Only gold members can continue reading. Log In or Register to continue