Fig. 9.1
Capillary malformation, face. a Hypertrophic lip with numerous ecstatic thin-walled venules on the superficial submucosa and thick-walled veins with prominent smooth muscle walls in a deeper submucosal location (arrows). b Superficial submucosal ecstatic thin-walled venules at higher magnification
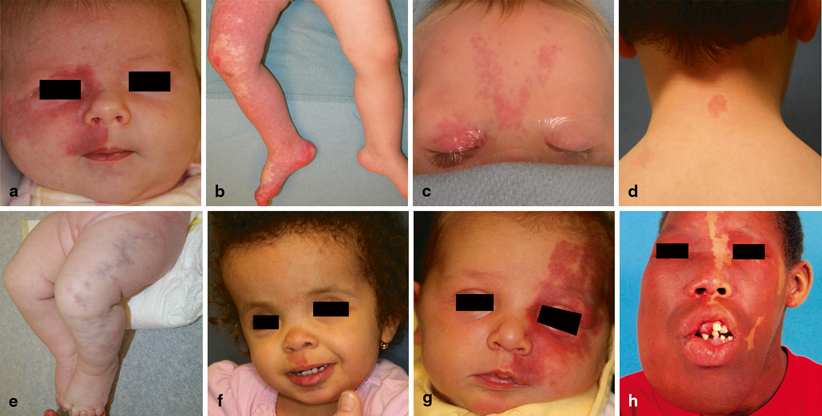
Fig. 9.2
Types of capillary malformation (CM). a 1-month-old girl with a sporadic CM. b Diffuse lower extremity CM with overgrowth in a 2-year-old boy. c Six-month-old boy with fading capillary stain of the forehead and right eyelid. d Three-year-old boy with a capillary malformation-arteriovenous malformation (CM-AVM) of the posterior neck exhibiting fast flow and a peripheral halo. e Three-month-old girl with cutis marmorata telangiectatica congenita (CMTC). Note the serpiginous and discolored craters of the left extremity. f Two-year-old girl with macrocephaly, frontal bossing, and CM of the philtrum—typical features of macrocephaly-capillary malformation (M-CM). g Two-week-old girl with Sturge-Weber syndrome. h Sixteen-year-old boy with Sturge-Weber syndrome showing soft-tissue and osseous overgrowth
Key Points
Most CMs are small and sporadic, and do not require treatment.
CMs may represent an underlying syndrome.
Pulse dye laser (PDL) is the primary treatment for CMs .
Most CMs can be managed by a single specialist, although syndromic patients or those with significant overgrowth are best managed in a vascular anomalies center by a multidisciplinary team.
Biology and Epidemiology
Pathophysiology
The pathogenesis of CM is not understood. Stasis in dilated, thin-walled channels may cause progressive vascular ectasia and soft-tissue thickening [4, 5]. Cobblestoning may be due to a lack of neural control of blood flow [6–8], or a loss of connective tissue support of the vessel wall [4, 9].
The mechanism of osseous overgrowth is unknown. It may be secondary to increased blood flow, the production of localized growth factors, or intraosseous CM [2].
Molecular/Genetic Pathology
CM-AVM is an autosomal dominant condition that results from a loss-of-function mutation in RASA1, which encodes p120RasGAP. This protein inhibits RAS p21 control of cellular proliferation, differentiation, and survival [10].
The etiologies of CMTC, M-CM, and SWS are unclear; they occur sporadically [3].
Incidence and Prevalence
Age Distribution
CM is present at birth.
Risk Factors
Relationships to Other Disease States, Syndromes
Parkes-Weber syndrome (PWS) is a diffuse arteriovenous malformation (AVM) in an overgrown extremity with an overlying CM [17].
Klippel-Trénaunay syndrome (KTS) consists of a capillary-lymphatic-venous malformation (CLVM) of an extremity in association with soft-tissue and/or skeletal overgrowth [2].
Presentation
Fading Capillary Stain
Vascular stain that resolves during early childhood [3].
Popularly referred as “angel kiss” when located on the forehead and “stork bite” when on the occipital scalp/posterior neck.
Capillary Malformation
CM is present at birth; however, the stain may not be evident because it can be hidden by the erythema of neonatal skin.
Facial CMs are associated with hypertrophy of the lip, cheek, or forehead; the lip is most commonly affected [2].
Fibrovascular nodules with cutaneous thickening and cobblestoning occur in 10–24 % of patients with nonsyndromic CM, especially when located in the second and third trigeminal nerve distribution [18–20].
Eighteen percent of patients develop pyogenic granulomas (PG) within the CM [2].
Enlargement of the maxilla or mandible can cause occlusal cant (vertical maxillary overgrowth) with increased dental show and malocclusion [2].
Capillary Malformation-Arteriovenous Malformation
The CM is typically nonproblematic; however, 30 % of patients have AVMs that can cause major morbidity: PWS (12 %), extracerebral AVM (11 %), or intracerebral AVM (7 %) [16].
An individual may have multiple CMs; however, 6 % of patients have a single lesion [16].
Five percent of patients have benign or malignant tumors, most commonly involving the nervous system (neurofibroma, optic glioma, vestibular schwannoma) [16].
Cutis Marmorata Telangiectatica Congenita
Macrocephaly-Capillary Malformation
A reticular CM, commonly on the face, associated with developmental delay and neurologic abnormalities [25].
Sturge-Weber Syndrome
Consists of: (1) upper facial CM, (2) ocular abnormalities (e.g., glaucoma, choroidal vascular anomalies), and (3) leptomeningeal vascular malformation [26].
Approximately 6–10 % of patients with a CM in the V1 distribution have SWS [27].
Leptomeningeal vascular anomalies ipsilateral to the CM can cause seizures and developmental delay [26].
Differential Diagnosis for Capillary Malformations
Arteriovenous malformation (AVM)
Congenital hemangioma (CH)
Infantile hemangioma (IH)
Kaposiform hemangioendothelioma (KHE)
Lymphatic malformation (LM)
Venous malformation (VM)
Diagnosis and Evaluation
Physical Examination
Fading Capillary Stain
Findings:
Macular red stain, which typically resolves by 2 years of age.
Usually located on the eyelids, glabella, nose, philtrum, and posterior neck; stains on the face normally fade, but those in the nuchal area may persist [3].
Capillary Malformation
Findings:
CMs initially may have a bright pink, red, or violaceous color. Darkening and thickening occurs over time [2, 3].
Lesions are located in the extremity (43.9 %), head/neck (32.8 %), or trunk (23.3 %) [11].
Hand-held Doppler examination shows normal flow in CMs, while hemangiomas and arteriovenous malformations exhibit fast flow.
Capillary Malformation-Arteriovenous Malformation
Cutis Marmorata Telangiectatica Congenita
Findings:
The skin is depressed and has a purple, reticulated pattern.
The stain may be localized, segmental, or generalized.
Most frequently involves the extremities, is unilateral (65 %), and affects the lower limb (69 %) [21].
Macrocephaly-Capillary Malformation
Sturge-Weber Syndrome
Findings:
Facial CM with ocular abnormalities (e.g., glaucoma, choroidal vascular anomalies) and leptomeningeal vascular malformation [2, 26].
Refractory seizures, contralateral hemiplegia, and delayed motor and cognitive development may be observed in this condition.
Soft-tissue overgrowth is present in 55–70 % of patients: lip (28–64 %), cheek (14 %), and forehead (5–6 %) [2].
Skeletal hypertrophy affects 22–45 % of patients: mandible (6–17 %), maxilla (48–72 %), or both jaws (22–35 %) [2].
Patients with SWS can have extracraniofacial CM (29 %) and extremity hypertrophy (14 %) [2].
Laboratory Data
RASA1 gene testing confirms the diagnosis of CM-AVM. However, not all patients with CM-AVM clinically will have a RASA1 mutation, suggesting that unknown mutations in RASA1 or other genes may exist [16].
Imaging Evaluation
More than 90 % of CMs are diagnosed by history and physical examination; imaging is rarely necessary.
Ultrasonography (US):
Can be performed without sedation. CM-AVM may show fast flow.
Computed Tomography (CT):
May be used to assess osseous overgrowth.
Magnetic Resonance Imaging (MRI):
Pathology
Histopathological diagnosis of CM is rarely necessary. In young children, the malformation shows dilated capillaries in the superficial dermis [30]. With increasing age, ectatic, venular-like vessels become more prominent in the papillary and reticular dermis [30]. Vessel size and density increase with age [4, 30]. CM-AVM shows large, tortuous arteries, and dilated, thick-walled veins (see Fig. 9.1) [30].
Treatment and Outcomes
Nonoperative Management
Drug therapy for CMs is not available. Abnormal periorbital and choroidal vascularity in patients with SWS can cause glaucoma, often leading to blindness [2]. Ophthalmologic examination should be performed every 6 months until the age of 2, and yearly thereafter [3].
Seventy-five percent of patients with SWS have seizures, which typically manifest during infancy [31]. Anticonvulsant therapy and regular neurology follow-up is necessary [31]. Neurosurgical intervention may be required for patients with severe seizures, drug therapy failures, or if antiepileptic medication is contraindicated [32].
Laser Therapy
Pulsed Dye Laser (PDL)
Originally developed for selective ablation of vascular lesions, PDL (595 nm wavelength) is the primary therapy for CM [3]. The laser penetrates 0.75–1.2 mm and thus deeper and larger vessels may not be affected. The settings used are 0.45–1.5 m/s pulse duration, 6–10 J/cm2 fluence, and 7–10 mm spot size [3]. It is effective and has a low risk of scarring [3, 33–36]. Intervention with PDL during early childhood is recommended because: (1) superior lightening of the lesion is achieved [37, 38], (2) the risk of darkening and hypertrophy is reduced [37], and (3) psychosocial morbidity is minimized. Multiple treatments, 6 weeks apart, are often required until the CM fails to improve [3].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


