the triple negative breast cancer may be tested as well. More information on BRCA1 and BRCA2 may be found in Chapter 21. Other less common genetic syndromes that confer elevated breast cancer risk are Cowden syndrome, Li-Fraumeni syndrome, Peutz-Jeghers syndrome, ataxia-telangiectasia heterozygosity, and hereditary diffuse gastric cancer.16
TABLE 16.1 Key Components to the Initial Evaluation of Breast Problems | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 16.2 Risk Assessment for Breast Cancer | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
dermal lymphatics by tumor can be easily visualized. In addition, local erythema of the breast which can be caused by cellulitis, mastitis, or an abscess can be differentiated from inflammatory breast cancer, which usually presents as diffuse erythema and edema of the breast. However, diagnosis will require biopsy for inflammatory breast cancer.
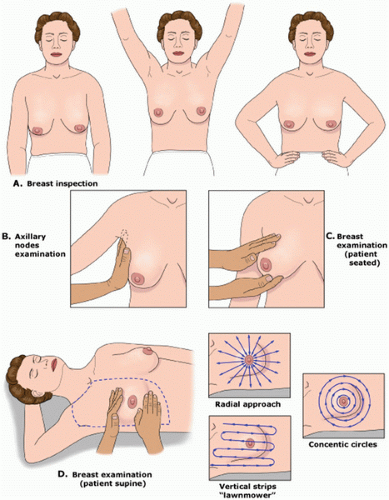 FIGURE 16.1 Clinical breast examination. A: The breast exam is started with the patient in a seated position with her arms relaxed. Breast inspection is aided by patient positioning. The patient is asked to raise her arms over her head so the lower part of the breasts can be inspected for asymmetry, skin changes, and nipple inversion or retraction. The patient then puts her hands on her hips and presses in to contract the pectoral muscles so that any other areas of retraction can be visualized. B: The regional lymph node exam is completed while the patient is still in the sitting position and includes the cervical, supraclavicular, infraclavicular, and axillary nodal basins. C: A bimanual examination of the breasts can be performed while the patient is still in the sitting position. This is especially useful for women with large pendulous breasts. D: The breast exam is completed with the patient in a supine position with the ipsilateral arm raised above her head. The area examined should extend from the clavicle superiorly to the rib cage inferiorly and from the sternum medially to the midaxillary line laterally. A systematic approach ensures that the entire breast is examined. This can be accomplished with either concentric circles, a radical approach, or vertical strips, referred to as the “lawnmower” method. (From Sabel MS. Breast masses and other common breast problems. UpToDate Web site. http://www.uptodate.com/contents/breast-masses-and-other-common-breast-problems. Accessed December 2, 2013.) |
triangulate the exact location of the abnormality and spot compression views over the area of interest which allow for greater compression, displacing the overlying breast tissue that could obscure a lesion.
TABLE 16.3 The American College of Radiology Breast Imaging Reporting and Data System | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
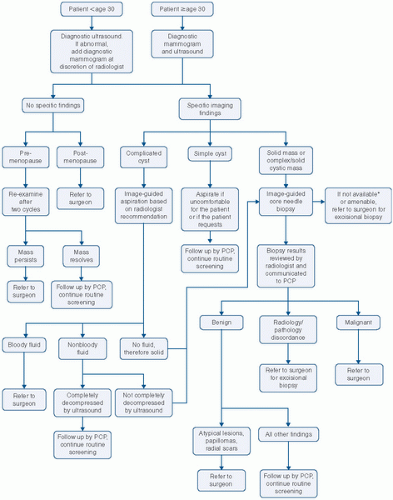 FIGURE 16.2 Algorithm for the management of a breast mass. PCP, primary care provider. |
age of 35 and 50 years and is extremely unusual in postmenopausal women not on estrogen replacement.
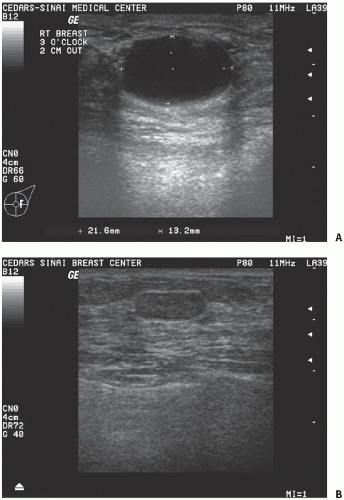 FIGURE 16.3 A: Ultrasound demonstrating a simple cyst. B: Ultrasound demonstrating a solid mass. |
breast cancer.96 Research has focused on abnormal levels of estradiol, progesterone, and prolactin as possible causes of mastalgia; however, no consistent findings have been observed.97, 98, 99 Inflammatory cytokines, interleukin-6, and tumor necrosis-α have also been implicated; however, no differences in expression have been seen in breast tissue from women who have no pain when compared to breast tissue from women who have mastalgia.100
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


