Chapter 694 Bone Structure, Growth, and Hormonal Regulation
Also see Chapters 48 and 564.
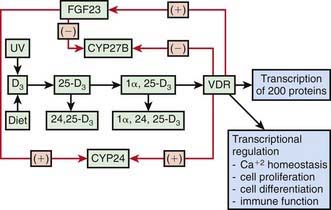
Rates of bone formation are coordinated with alterations in mineral metabolism in both the intestine and kidneys. Inadequate dietary intake or intestinal absorption of calcium causes a fall in serum levels of calcium and its ionized fraction. This serves as the signal for PTH synthesis and secretion, resulting in greater bone resorption to raise the serum calcium level, enhanced distal tubular reabsorption of calcium, and higher rates of synthesis by the kidneys of 1,25(OH]2D or calcitriol, the most active metabolite of vitamin D (Fig. 694-1). Calcium homeostasis thus is controlled by the intestine because the availability of 1,25(OH)2D ultimately determines the fraction of ingested calcium that is absorbed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


