Biopsy in Pregnancy: Risks, Benefits, Pathologic Findings, and Illustrative Examples
Fig. 7.1
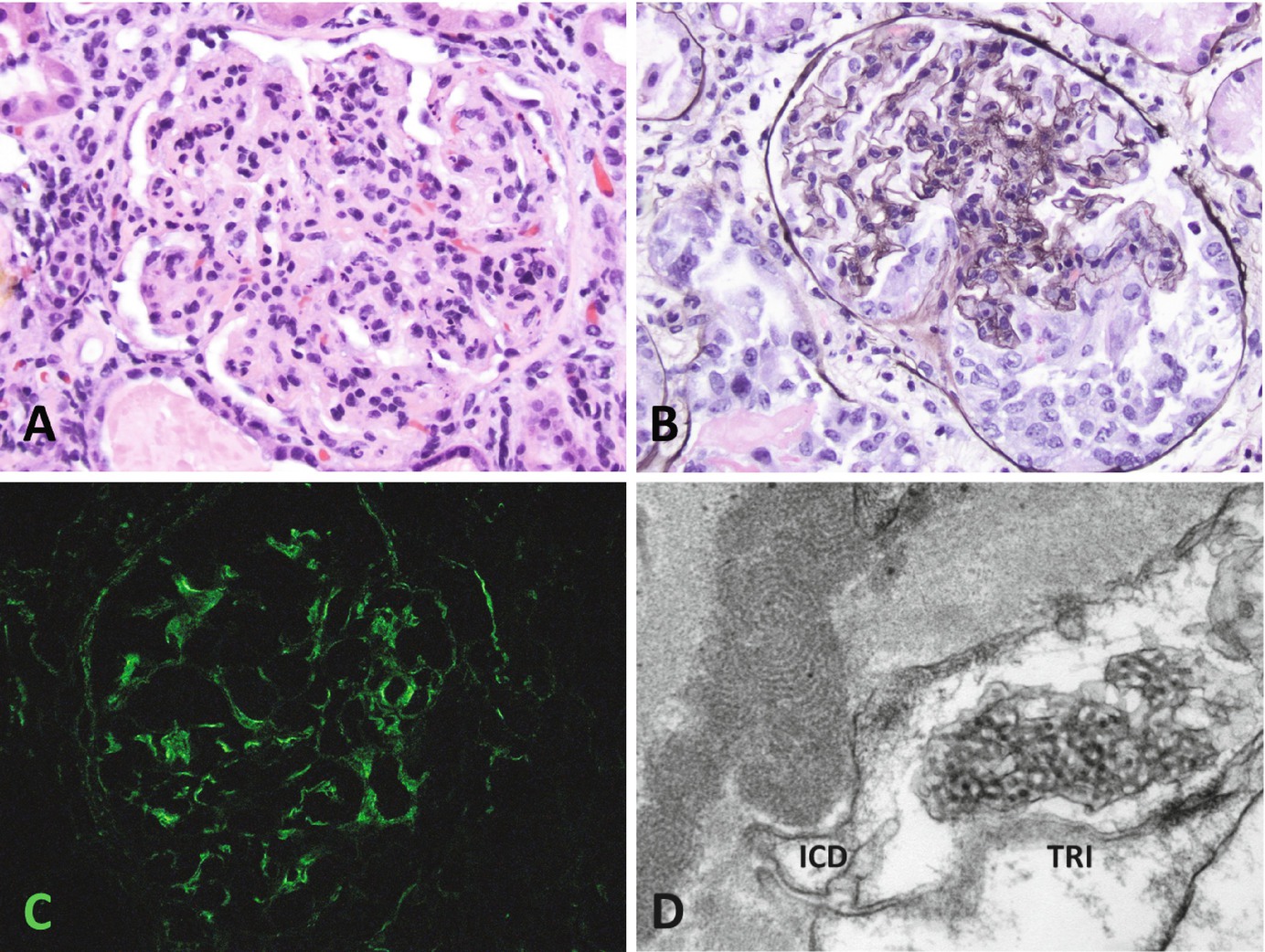
Endotheliosisin preeclampsia. (a) Enlarged glomeruli with enhanced lobulation. Hematoxylin and eosin, 200×. (b) Glomerular capillaries filled and distended with swollen, pale endothelial cells, imparting a “bloodless” appearance. PAS stain, 200×. (c) Glomerular basement membranes with double contours. Jones silver methenamine stain, 400×. (d) Electron microscopy showing swollen endothelial cells (arrows) filling capillary lumens, but without deposits, 2700×
Endothelial cell swellingis not accompanied by a significant influx of inflammatory cells, a feature that distinguishes PEC from immune complex or complement-mediated diseases such as membranoproliferative glomerulonephritis (MPGN), postinfectious glomerulonephritis, and others. Capillary walls are frequently thickened and may occasionally have double contours and mesangial interposition [26], a feature shared with MPGN. Intraglomerular foam cells may be present, similar to those seen in other nephrotic diseases such as focal segmental glomerulosclerosis. The mesangium may be expanded and hypercellular, but usually not to the degree that can be seen in proliferative glomerulonephritis such as lupus nephritis(Fig. 7.2), IgA nephropathy, or MPGN (not shown). Crescents are rarely seen and usually correlate with clinically severe disease [30].
Fig. 7.2
Active lupus nephritis. (a, b) Glomeruli are hypercellular, but endothelial cells are less swollen and neutrophils are present. In this case, a crescent is present. This is sometimes seen in lupus nephritis but is rare in preeclampsia. (a) Hematoxylin and eosin, 200×. (b) Jones silver methenamine, 200×. (c) IgG immunostaining of mesangium, capillary walls, and Bowman’s capsule; similar staining also present for IgA, C3, C1q, kappa, and lambda (not shown). Immunofluorescence 200×. (d) Immune complex deposits in the mesangium and subendothelial areas with “fingerprint” structure and tubuloreticular inclusions in endothelial cells. (Electron microscopy, 40,000×)
Immunofluorescence may show a wide variety of patterns, none of which are specific to preeclampsia. Fibrinogen and IgM are most commonly seen, but other immune components including IgG and complement have been reported [31, 32].
Electron microscopy confirms and extends the light microscopic findings [3, 4]. Endothelial swellingis always present, as often are increased numbers of mesangial cells and glomerular basement membrane (GBM) duplication with mesangial interposition, which accompany many types of endothelial injury (Fig. 7.1d). Vaguely defined subendothelial and mesangial densities may be present and correlate with fibrinogen seen by immunostaining. Segmental podocyte foot process effacement can be seen with or without the light microscopic lesion of focal and segmental glomerulosclerosis(FSGS). As in other renal diseases, podocyte foot process effacement correlates with proteinuria, though not always quantitatively with the degree of proteinuria [33].
Glomerular changespersist for only a short time after delivery. The light microscopic lesion of endotheliosis usually regresses within 2–3 months, sometimes as little as 2–3 weeks [34], while electron microscopic findings may disappear within days [26]. This change correlates with the typically rapid resolution of clinical disease postpartum.
Other pathologic entities may coexist with PEC in pregnancy and may be clinically confused with it. In some clinical situations biopsy may be necessary to clarify the diagnosis and allow for appropriate treatment. The most frequent of these is the histologic lesion of FSGS(Fig. 7.3), which may be present in pregnancy and accompany PEC. Since the clinical entity of primary FSGS typically produces proteinuria, it may be mistaken for PEC. It remains unresolved whether histologic FSGS in pregnancy is part of a physiologic response to hyperfiltration, related to PEC, or a manifestation of other pre-existing or de novo renal diseases. Patients with PEC and FSGS tend to have a more severe course than those with PEC alone, including more pronounced hypertension and full-blown nephrotic syndrome. Even so, proteinuria tends to resolve within a few months after delivery, and persistent hypertension is uncommon [35, 36].
Fig. 7.3
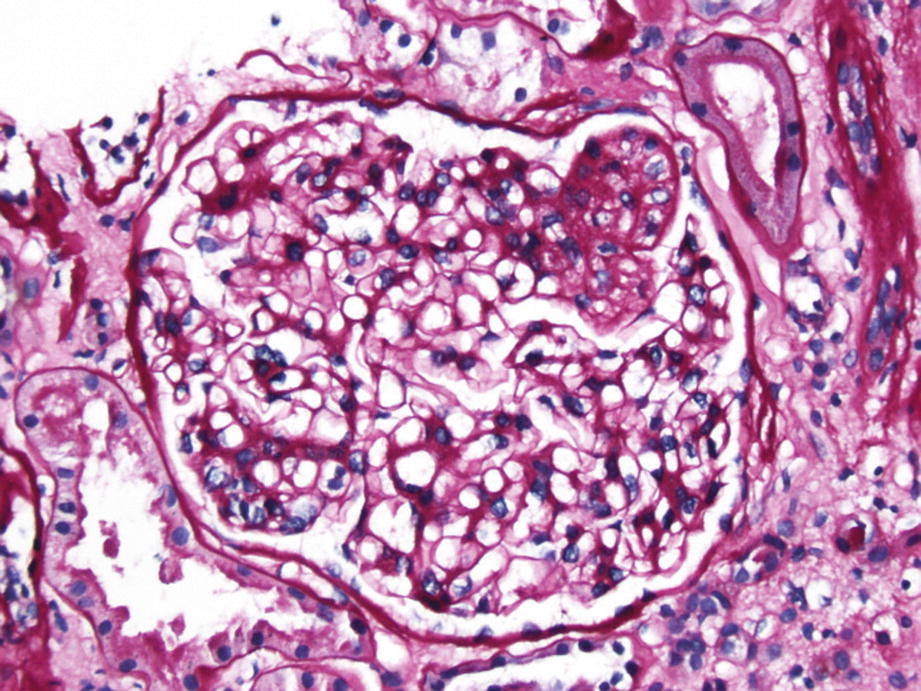
Focal and segmental glomerulosclerosis. A portion of the glomerulus (2 o’clock position) shows consolidation with closure of capillary loops (PAS stain, 200×)
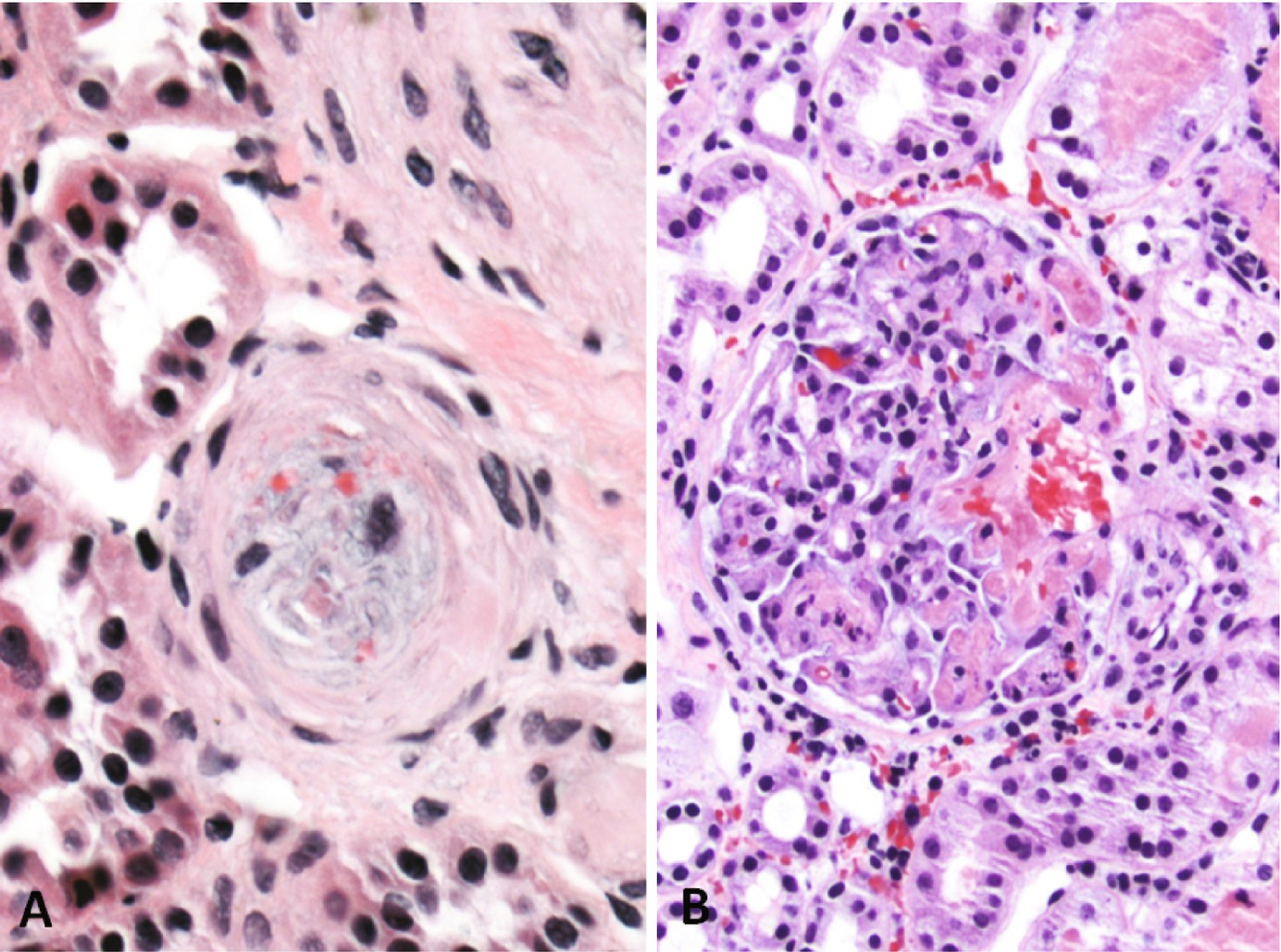
Non-glomerular changes often seen in PEC are not specific to that process. There may be tubulointerstitial inflammation and/or atrophy. When seen, concurrent interstitial nephritis or an underlying chronic process should be considered. Arterial intimal fibrosis (Fig. 7.4) may be a marker of pre-existing hypertensive nephropathybut can be seen in non-PEC pregnancy-related hypertension as well. In contrast to malignant hypertension, thrombosis and arteriolar “onion skinning” are not typically reported in association with preeclampsia.
Fig. 7.4
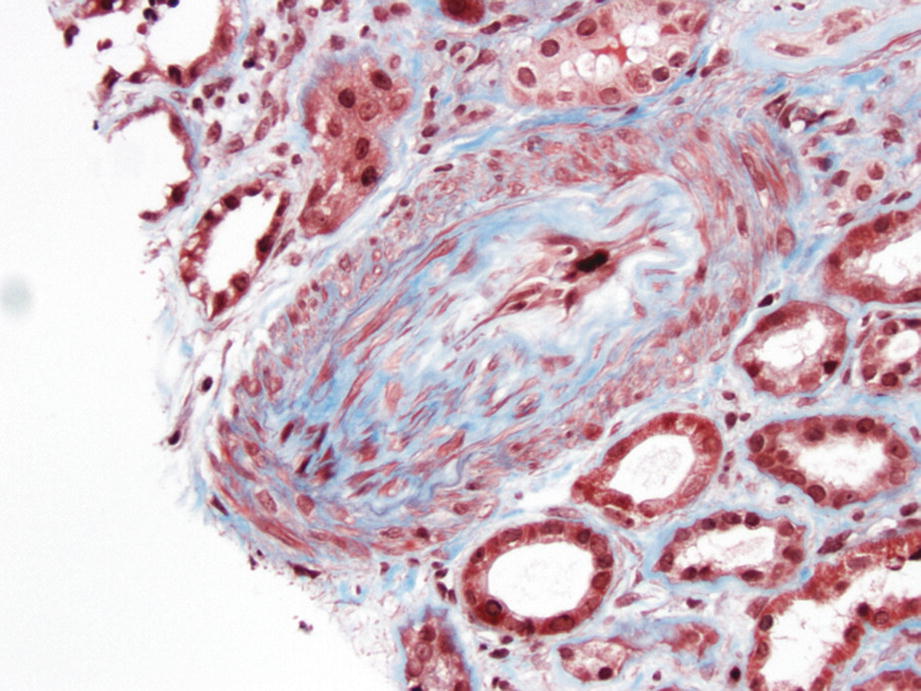
Hypertensive renovascular disease. An artery with severe intimal fibrosis in a case of long-standing hypertension. Fibrosis is not seen in hypertension of new onset, such as in preeclampsia. (Trichrome stain, 200×)
Acute Tubular Necrosis
Acute tubular necrosis (ATN)can be seen (Fig. 7.5), which may or may not be related to PEC. Features of ATN include tubular dilatation and epithelial attenuation; more severe cases may show sloughing of tubular epithelium and reparative mitotic activity.
Fig. 7.5
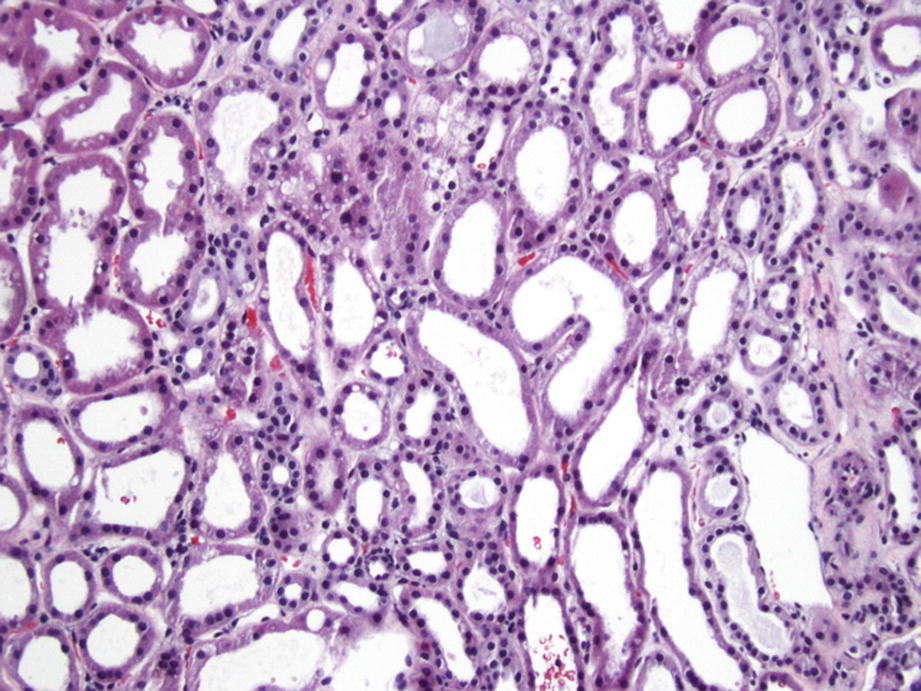
Acute tubular injury/necrosis. Tubules are dilated with epithelial attenuation (flattening). In more severe cases, cells may detach from basement membrane. (Hematoxylin and eosin, 100×)
Thrombotic Microangiopathy
Thrombotic microangiopathy (TMA)in pregnancy can be seen with or without concurrent PEC. The underlying lesion of TMA, microvascular injury, is similar to that of PEC, which is reflected in their common morphologic pattern of endothelial cell swelling. However, in contrast to PEC, TMA is characterized by fibrin thrombi within glomerular capillaries and extraglomerular arterioles (Fig. 7.6). Glomerular involution due to ischemia is a common finding in TMA, as is secondary ATN due to downstream hypoxia from glomerular capillary occlusion. Acute fatty liver of pregnancy has renal features that overlap to some degree with ATN and TMA, with the additional finding of fatty vacuolization of tubular epithelial cells.
Fig. 7.6
Thrombotic microangiopathy. (a) Arterioles are occluded by fibrin and fragmented red blood cells, with endothelial swelling. (Hematoxylin and eosin, 400×). (b) Glomerular capillaries are distended by fibrin thrombi. (Hematoxylin and eosin, 200×)
Only gold members can continue reading. Log In or Register to continue