Source
Information
Clinical history
Pain
Tripping
In-/Out-toeing
Physical examination
Gross foot shape weight-bearing/non weight-bearing
Flexible/rigid
Plantar callous pattern
Radiographic examination
Segmental alignment weight-bearing, AP and LAT views
Observational gait analysis
Foot contact with floor (3 rockers)
Foot progression angle
Foot clearance in swing phase
Quantitative gait analysis
Kinematics
Kinetics
Dynamic EMG
Pedobarography
This chapter will begin with an overview of normal ankle and foot function during the gait cycle. This will provide a framework for the identification of common (or coupled), and uncommon (or uncoupled), segmental malalignments of the ankle and foot. This will be followed by an overview (principles and indications) of the most common interventions (i.e., soft tissue surgery, guided growth, osteotomies, and arthrodeses) utilized to correct these segmental malalignments. Finally, a standardized approach for the preoperative, intraoperative, postoperative, and surveillance of ankle and foot alignment and function will be presented.
Ankle and Foot Function During Normal Gait
The understanding of ankle and foot function during normal gait is facilitated by considering the lower leg to consist of four segments: the tibial or shank segment, the hindfoot (talus and calcaneus), the midfoot (navicular, cuneiforms, and cuboid), and the forefoot (metatarsals and phalanges) [1–3, 5, 6] (Fig. 10.1a, b). It is also helpful to consider the foot to consist of two columns: the medial column (talus, navicular, cuneiforms, great toe metatarsal, and phalanges), and the lateral column (calcaneus, cuboid, lesser toe metatarsals, and phalanges) [7] (Fig. 10.2a–c). Standardized, consistent terminology is required to describe the alignment of the separate segments of the ankle and foot [8]. Movement of the plantar aspect of the segment in question during the gait cycle is described as inversion (towards the midline) or eversion (away from the midline). Movement of the distal aspect of the segment in question during the gait cycle is described as adduction (towards the midline) or abduction (away from the midline). Supination is a combination of inversion and adduction. Pronation is a combination of eversion and abduction. Rotation of the segment about its longitudinal axis towards the midline is described as internal rotation. Rotation of the segment about its longitudinal axis away from the midline is described as external rotation.
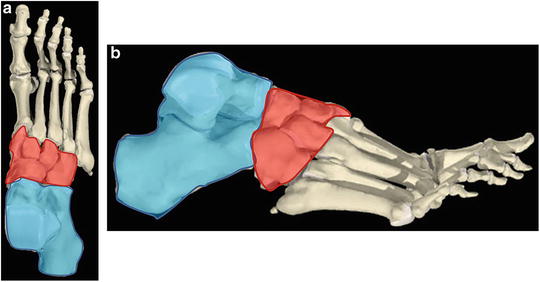
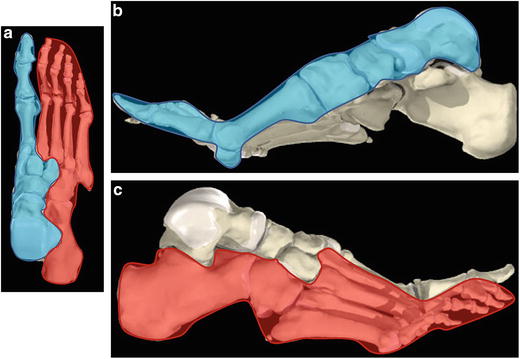
Fig. 10.1
Three segments of the foot. (a) Diagram of the anteroposterior view of the right foot. The hindfoot segment is blue, the midfoot segment is red, and the forefoot segment is white. (b) Diagram of the lateral view of the right foot. The hindfoot segment is blue, the midfoot segment is red, and the forefoot segment is white
Fig. 10.2
Two columns of the foot. (a) Diagram of the anteroposterior view of the right foot. The medial column is blue, and the lateral column is red. (b) Diagram of the lateral view (medial side) of the right foot. The medial column is blue. (c) Diagram of the lateral view (lateral side) of the right foot. The lateral column is red
The gait cycle is a period of time beginning with the initial contact of the reference foot with the ground, continuing through ipsilateral stance and swing phases until the subsequent ipsilateral initial contact. Stance phase occurs when the reference limb is in contact with the ground. Swing phase occurs when the reference limb is not in contact with the ground. The interaction of the ankle and foot with the ground during the stance phase of the gait cycle is described by the concept of three rockers [2, 3]. In normal gait, the heel is the first part of the foot to contact the ground at initial contact. The ankle subsequently plantar flexes until the foot is flat on the floor. This motion is controlled by the eccentric activity of the ankle dorsiflexor muscle group. The first, or heel rocker, occurs from heel strike to foot flat during the loading response subphase of stance. As the body progresses forward, the tibia advances forward over the foot, which is achieved by ankle dorsiflexion. This motion is controlled by eccentric activity of the ankle plantar flexor muscle group. The second, or ankle rocker, occurs as the tibia advances over the foot during the midstance subphase of stance. Immediately prior to the initial contact of the opposite foot, the heel of the reference foot rises off the ground and dorsiflexion occurs through the metatarsophalangeal joints of the forefoot. This motion is controlled by concentric activity of the ankle plantar flexor muscle group. The third, or forefoot rocker, occurs as the ankle begins to plantar flex during the terminal stance subphase of stance. This is an essential event during normal gait, as the largest moment generated by any single muscle group during the gait cycle is the internal plantar flexion moment generated by the ankle plantar flexor muscle group during third rocker in terminal stance [2, 3, 9].
In the stance phase of the normal gait cycle, the ankle and foot provide shock absorption during loading response (first or heel rocker), stability during midstance (second or ankle rocker), and a rigid lever during terminal stance (third or forefoot rocker) [2, 3]. During loading response, the tibial or shank segment rotates internally, and the ankle is plantarflexing (Fig. 10.3a). This results in eversion and abduction of the hindfoot, primarily through the subtalar joint (see Fig. 10.3b, c). Pronation of the hindfoot forces the talus to plantarflex, which “unlocks” the joints of the midfoot, which follows into pronation (see Fig. 10.3d, e) This coupled movement of the hindfoot and midfoot results in maximum flexibility of the foot, which allows the joints to contribute to shock absorption. During midstance, the tibial or shank segment is rotating externally, and the ankle is dorsiflexing (Fig. 10.4a). This results in inversion and adduction of the hindfoot, primarily through the subtalar joint (see Fig. 10.4b, c). Supination of the hindfoot forces the talus to dorsiflex, which “locks” the joints of the midfoot, which follows into supination (see Fig. 10.4d, e) This coupled movement of the hindfoot and the midfoot results in restoration of the longitudinal arch of the foot and maximum rigidity of the foot, which enhances stability. During terminal stance, the tibial or shank segment continues to rotate externally, and the ankle continues to dorsiflex. As the body progresses forward, the center of pressure beneath the foot advances distally into the forefoot. Because the segments of the foot are aligned to promote maximum rigidity, the forefoot is stable as it is loaded. The rigidity of the foot segments provides an optimal lever arm to the ankle plantar flexor muscles during terminal stance. Normal, expected segmental alignment patterns of the ankle and foot during the stance phase of the gait cycle, as described above, are the consequence of coupled movements between the anatomical segments.
Fig. 10.3
Skeletal alignment of the lower extremity during the first rocker of stance phase. (a) The tibia is rotating internally (red arrow) and the ankle is plantarflexing (blue arrow). (b) Hindfoot alignment during the first rocker of stance phase consists of calcaneal eversion (red arrow). (c) Hindfoot alignment during the first rocker of stance phase consists of calcaneal abduction (red arrow). (d) Hindfoot pronation (eversion and abduction) forces the talus to plantarflex (red arrow) during the first rocker of stance phase. (e) This “unlocks” the primary joints of the midfoot (talo-navicular in solid circle, calcaneocuboid in dashed circle). (f) Coronal view of the articulation between the hindfoot and midfoot in first rocker of stance phase. Lateral is to the left, medial is to the right. TNJ talo-navicular joint, CCJ calcaneocuboid joint, Calc calcaneus. The main axes of the TNJ and CCJ are parallel (red lines), which allows motion and “unlocks” the midfoot
Fig. 10.4
Skeletal alignment of the lower extremity during the second rocker of stance phase. (a) The tibia is rotating externally (red arrow) and the ankle is dorsiflexing (blue arrow). (b) Hindfoot alignment during the second rocker of stance phase consists of calcaneal inversion (red arrow). (c) Hindfoot alignment during the second rocker of stance phase consists of calcaneal adduction (red arrow). (d) Hindfoot supination (inversion and adduction) forces the talus to dorsiflex (red arrow) during the second rocker of stance phase. (e) This “locks” the primary joints of the midfoot (talo-navicular in solid circle, calcaneo-cuboid in dashed circle). (f) Coronal view of the articulation between the hindfoot and midfoot in second rocker of stance phase. Lateral is to the left, medial is to the right. TNJ talo-navicular joint, CCJ calcaneocuboid joint, Calc calcaneus. The main axes of the TNJ and CCJ are no longer parallel (red lines), which restricts motion and “locks” the midfoot
In the swing phase of the normal gait cycle, the foot and ankle contribute to clearance and pre-positioning for the subsequent stance phase [2, 3, 6]. During pre- and initial swing the tibia or shank segment is rotating externally and the ankle is plantar flexing. The segments of the foot are “unlocked” as the limb is unloaded. During mid swing the tibia or shank segment is rotating internally and the ankle is dorsiflexing. These coupled motions serve to functionally shorten the limb and promote clearance. During terminal swing these coupled motions continue and the foot is maintained in a plantigrade alignment, perpendicular to the anatomical axis of the tibia or shank segment. This pre-positioning of the foot during terminal swing will result in a heel strike at the initial contact, which is the optimal alignment for the ankle and foot as the extremity enters the subsequent stance phase in loading response.
Box 10.1
The lower leg consists of four segments: the tibial or shank segment, the hindfoot (talus and calcaneus), the midfoot (navicular, cuneiforms and cuboid), and the forefoot (metatarsals and phalanges).
The interaction of the ankle and foot with the ground during the stance phase of the gait cycle is described by the concept of three rockers; first or heel rocker, second or ankle rocker, and third or forefoot rocker.
In the stance phase of the normal gait cycle, the ankle and foot provide shock absorption during loading response (first or heel rocker), stability during midstance (second or ankle rocker), and a rigid lever during terminal stance (third or forefoot rocker).
In the swing phase of the normal gait cycle, the foot and ankle contribute to clearance and pre-positioning for the subsequent stance phase.
Segmental Malalignment Patterns of the Ankle and Foot
Segmental malalignments of the ankle and foot may be categorized as coupled or uncoupled. Coupled segmental malalignments represent exaggerations of normal segmental alignments that occur during the gait cycle (as described above). The three most common coupled segmental malalignments are equinus, equinoplanovalgus, and equinocavovarus. Equinus is characterized by excessive plantar flexion of the hindfoot relative to the ankle, with normal midfoot and forefoot alignment (Fig. 10.5a, b) Equinoplanovalgus is characterized by equinus deformity of the hindfoot, coupled with pronation deformities of the midfoot and forefoot (Fig. 10.6a, b). The lateral column of the foot is functionally and/or structurally shorter than the medial column. Ankle valgus and hallux valgus deformities are frequently seen in association with equinoplanovalgus foot segmental malalignment (see Fig. 10.6c, d) Equinocavovarus is characterized by equinus deformity of the hindfoot, coupled with supination deformity of the midfoot and variable malalignment of the forefoot (Fig. 10.7a, b) The lateral column is functionally and/or structurally longer than the medial column. Compensatory ankle valgus deformity may be seen in association with equinocavovarus foot segmental malalignment.
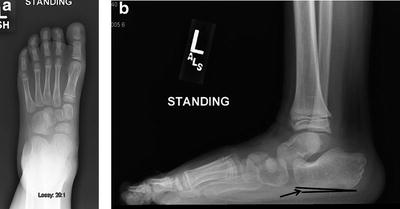


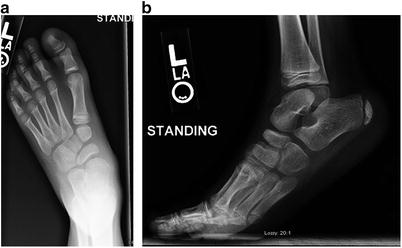
Fig. 10.5
Plain radiographs of the foot in a child with equinus deformity. (a) Anteroposterior view shows normal segmental alignment. (b) Lateral view shows hindfoot plantarflexion (diminished calcaneal pitch, indicated by solid arrow towards angle formed by solid lines, normal is approximately 20°), with otherwise normal segmental alignment
Fig. 10.6
Plain radiographs of the foot in a child with equinoplanovalgus deformity. (a) Anteroposterior view shows hindfoot pronation, talonavicular uncoverage, forefoot abduction and hallux valgus. (b) Lateral view shows hindfoot plantarflextion, midfoot pronation (excessive naviculocuboid overlap), and forefoot pronation (excessive overlap of the metatarsals). (c) Anteroposterior view of the ankle shows ankle valgus deformity (increased tibiotalar angle, lateral wedging of the distal tibial epiphysis, and a high fibular station). (d) Clinical photograph of the left hindfoot in weight-bearing for this child. There is significant hindfoot valgus deformity, which the radiographs show to be a consequence of both tibiotalar (ankle) and talo-calcaneal (subtalar) valgus malalignments
Fig. 10.7
Plain radiographs of the foot in a child with equinocavovarus deformity. (a) Anteroposterior view shows hindfoot supination (excessive overlap of the talus and calcaneus), and forefoot adduction (medial deviation of the great toe metatarsal relative to the talus). (b) Lateral view shows hindfoot varus (parallelism of the talus and calcaneus), midfoot supination (diminished naviculocuboid overlap), and forefoot supination (excessive stacking of the metatarsals)
In all three coupled segmental malalignment patterns, heel strike at initial contact does not occur, disrupting the first or hindfoot rocker and shock absorption function in loading response. Equinus and equinocavovarus malalignment patterns disrupt the second or ankle rocker by blocking ankle dorsiflexion, compromising stability function in midstance. Equinoplanovalgus malalignment maintains the mid- and forefoot segments in an “unlocked” alignment, compromising stability function in midstance, which may result in excessive loading of the plantar, medial portion of the midfoot. All three coupled segmental malalignments may compromise the ability of the ankle plantar flexor muscles to generate an adequate internal plantar flexion moment during third or forefoot rocker. The hindfoot malalignment associated with equinus and equinocavovarus malalignment patterns shortens the length of the plantar flexor muscles, compromising their ability to generate tension, as described by the length-tension curve for skeletal muscle [10, 11]. With equinoplanovalgus, the moment generating capacity of the ankle plantarflexor muscles is further compromised by the malalignment of mid-and forefoot segments, which effectively shortens the lever arm available to this muscle group during the third or forefoot rocker. All three segmental malalignment patterns of the ankle and foot may inhibit ankle dorsiflexion in swing phase, compromising clearance in midswing and proper positioning of the foot and ankle in terminal swing.
Uncoupled segmental malalignments are alignment patterns between the hind-, mid-, and forefoot that never occur during the gait cycle. Equinocavovalgus is an example of an uncoupled segmental malalignment pattern (Fig. 10.8a, b). Uncoupled segmental malalignments of the ankle and foot are relatively uncommon, and are frequently the consequence of deformity following previous surgery.